An aircraft launches on a legitimate emergency. The crew documents the transport, the patient reaches definitive care, and the clinical mission is done. Then the remittance arrives and the payment bears little resemblance to the operational cost, the urgency, or the complexity of the flight.
That's the operating reality many air ambulance providers are dealing with under the No Surprises Act. The patient is usually no longer the pressure point in out-of-network emergency air ambulance billing. The payer is. Revenue that used to be contested through balance billing is now fought over through claim adjudication, negotiation, and federal dispute resolution.
Introduction The New Reality for Air Ambulance Revenue
A flight launches at 2:14 a.m. The crew makes the transport decision with limited time, incomplete information, and a patient who cannot wait for payer rules to catch up. The mission ends at the receiving facility. The revenue risk starts when the claim hits the plan.
For air ambulance operators, the No Surprises Act changed where reimbursement pressure shows up. The law limits what patients pay for covered emergency out-of-network air ambulance services, but it does not settle what the payer owes the provider. The billing dispute did not disappear. It shifted into claims operations, appeals, negotiations, and federal dispute resolution.
Federal consumer guidance also makes clear that the law does not guarantee payment. If an insurer denies coverage for an air ambulance service, the patient may still face the full bill under the Department of Labor's surprise billing guidance. From an operator's perspective, that creates two parallel risks at once: underpayment from the plan and patient balance exposure if the claim is denied outright.
That shift has practical consequences inside revenue cycle. Dispatch intake, eligibility work, documentation, coding, and denial management now affect recoverability much earlier in the life of the claim. A weak record at intake usually becomes a weak position in appeal. A weak appeal file usually becomes a harder IDR case.
Three capabilities separate operators that preserve yield from operators that spend months reacting to payer behavior:
- Clean front-end intake: plan identification, coverage screening, and demographic accuracy before preventable errors get baked into the claim
- Clinical documentation built for review: records that support urgency, patient condition, interventions, and why the air transport was appropriate at the time of service
- Post-payment discipline: a defined process for reviewing initial payments, spotting underpayment patterns, and escalating cases fast enough to protect filing and dispute deadlines
The financial stakes are high because these are expensive, heavily scrutinized claims. Air ambulance leaders should treat NSA compliance as a core revenue strategy issue, not an isolated legal task. The operators that recover more cash under the NSA usually connect operations, clinical charting, coding, payer strategy, and IDR preparation into one working model.
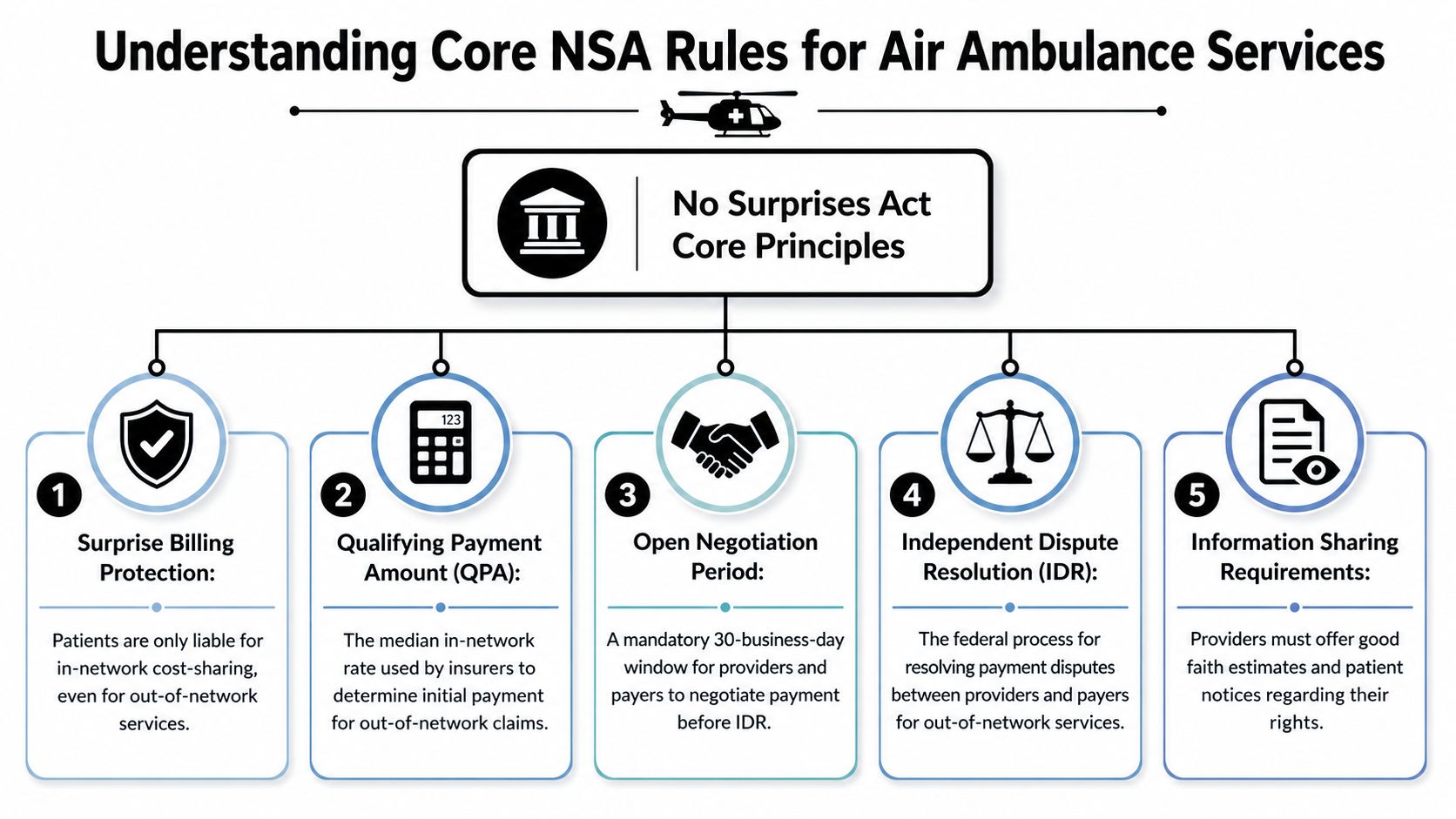
Understanding Core NSA Rules for Air Ambulance Services
A flight goes out on an emergency pickup, the crew does everything right, and the claim still comes back with patient cost-sharing capped and the plan paying far less than the operator expected. That is the revenue reality the No Surprises Act created for air ambulance providers.
For covered emergency out-of-network air ambulance services, the patient's cost-sharing is limited to the in-network amount, and those amounts count toward the plan's in-network deductible and out-of-pocket maximum under the ASPE air ambulance issue brief.
For operators, the practical effect is simple. The patient is no longer the fallback source for the unpaid balance on covered emergency claims. If the plan underpays, revenue recovery has to come from claim accuracy, documentation strength, negotiation discipline, and, when needed, formal dispute action against the payer.
What the balance billing ban changes operationally
The ban on balance billing is usually framed as a patient protection rule. For providers, it is also a cash flow rule.
Under the old model, some organizations could offset part of a payment shortfall by billing the patient for the remaining balance, subject to state law and contract limits. Under the NSA, that option is generally off the table for covered emergency air ambulance transports. The financial disagreement stays between the provider and the health plan.
That changes the operational priorities inside revenue cycle:
- Identify the right plan and funding type early
- Confirm the transport falls within NSA-protected emergency service rules
- Submit a clean claim with complete clinical support
- Review the initial payment and any notice explaining the payer's position
- Escalate quickly if the amount is not commercially reasonable
Each step affects recoverability. A weak intake file creates coverage questions. A weak chart gives the payer room to challenge medical necessity, urgency, or transport appropriateness. A delayed review of the initial payment can push the account too close to negotiation and dispute deadlines.
How the QPA affects payment strategy
The Qualifying Payment Amount, or QPA, appears in many NSA air ambulance disputes because payers often use it to support their initial out-of-network payment position. Providers should understand what that number is and what it is not.
The QPA is the plan's benchmark, calculated under the statute and regulations. It is not a statement of the operator's actual cost to maintain aircraft, crews, readiness, clinical capability, and response coverage. It also does not automatically reflect difficult geography, low-volume bases, specialty transport capacity, or mission-specific complexity.
That gap matters in practice. I have seen operators treat the first payment as if the plan had already made its final valuation decision. That is a mistake. The initial payment often serves as the payer's anchor, not the last word on value. Revenue teams need to test the payer's rationale, preserve the record, and build the case for why the payment does not reflect the service that was delivered.
The question after the NSA is no longer whether the patient can be billed for the difference. The question is whether the provider can document and defend a higher payment from the plan.
Why air ambulance remains a pressure point under the NSA
Air ambulance claims draw scrutiny for reasons every operator recognizes. The claims are expensive, medically urgent, and less familiar to many commercial plans than routine facility or professional claims. That combination often produces aggressive review behavior, narrow payment positions, and heavy reliance on payer benchmarks.
The legal timeline matters, but the business impact matters more. The statute was signed on December 27, 2020, and the federal protections took effect on January 1, 2022. Air ambulance services were included from the start. For providers, that did not reduce reimbursement friction. It changed the forum. What used to be a patient balance problem became a payer dispute problem, and that is a very different operating model.
Operators that do well under the NSA usually treat these rules as payment mechanics, not just compliance language. They train intake, coding, billing, and appeals teams to see the same claim the way a payer reviewer or IDR entity will see it later. That shift is what turns the NSA from a margin threat into a recoverable revenue process.
A Provider's Guide to the IDR Process
A transport goes out at 2:00 a.m. The crew handles a high-acuity transfer, the chart supports medical necessity, and the claim is paid at a fraction of billed charges. Under the No Surprises Act, that shortfall no longer turns into a patient balance issue. It turns into a payer recovery problem, and for air ambulance operators, IDR is often where a meaningful part of that revenue is won or lost.
Federal IDR is not just a legal remedy. It is a revenue cycle process with legal deadlines attached. Teams that treat it as a late-stage appeal usually lose time, miss filing windows, or submit thin evidence. Teams that treat it as part of core RCM usually recover more because the dispute file, payment position, and deadline tracking are built into operations from the start.
Research on NSA air ambulance disputes has shown a wide gap between payer offers, provider offers, and final awarded amounts. That matters operationally. The initial payment is often only the payer's opening position, not a realistic measure of claim value, so operators need a disciplined method for deciding which accounts to advance and how aggressively to support them.
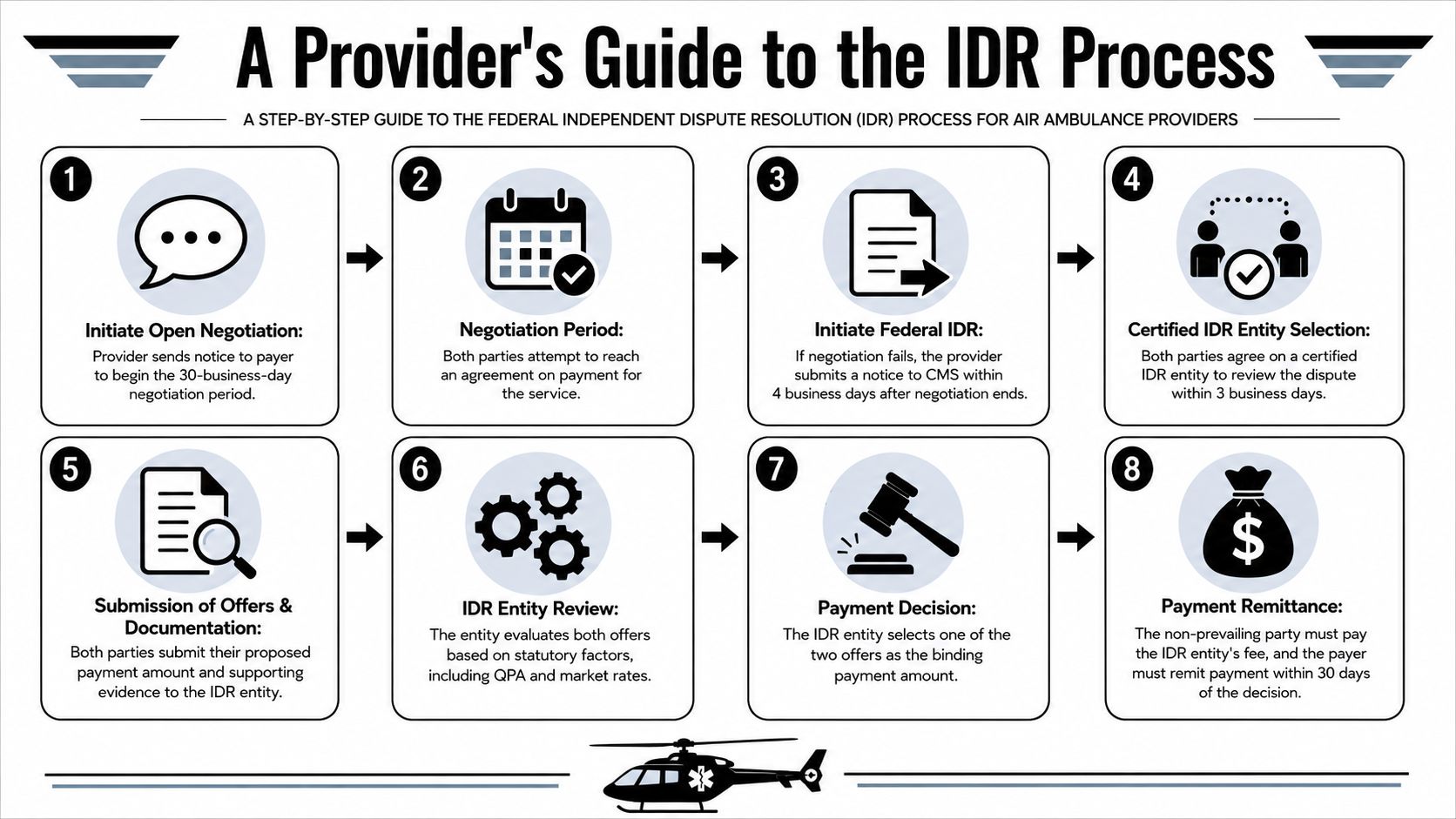
The sequence that affects payment recovery
The deadlines are short, and each handoff matters.
| Event | Deadline | Action Required by Provider |
|---|---|---|
| Open negotiation begins | 30 business days | Send notice and track all payer responses |
| Federal IDR initiation | Within 4 business days after negotiation ends | Submit the dispute notice on time |
| IDR entity selection | Within 3 business days | Coordinate selection and document communications |
| Offer and evidence submission | Per process requirements after entity selection | Submit a concise, evidence-backed payment position |
| Payment after decision | Within 30 days of decision | Monitor remittance and escalate nonpayment promptly |
In practice, the biggest failures are not usually legal arguments. They are process failures. A negotiation notice is not logged. The wrong remittance is attached. Someone assumes outside counsel has the file, while counsel assumes billing has already organized it.
For teams that need a clearer operating model, an air ambulance IDR workflow can help define ownership across billing, legal, and clinical review.
What belongs in the dispute file
A strong IDR submission gives the reviewer a payment rationale they can follow without guessing. That means the file has to do more than show that transport occurred.
Include the records that explain why the service justified the provider's offer:
- Clinical necessity support: Documentation should explain the patient's condition, the urgency of transport, and why air transport was appropriate for that point of care.
- Service-level operational facts: Aircraft type, crew configuration, interventions during transport, time factors, and origin-to-destination circumstances can all matter when the payer tries to flatten the claim into a generic benchmark.
- Payment history and adjudication record: Include the initial payment or denial, remittance details, open negotiation communications, and a clean calculation showing the gap between the plan's position and the provider's requested amount.
- Internal consistency: Coding, narratives, transport logs, PCS or transfer documentation, and correspondence should support the same story.
Air ambulance providers contend with a significant change under the NSA. The patient protection rules are settled. The harder question is whether the operator can convert a clinically valid mission into a well-supported payment claim that survives payer scrutiny and arbitration review.
How experienced operators use IDR strategically
Not every underpaid claim belongs in IDR. Filing fees, staff time, evidence preparation, and follow-up costs are real. Operators get better results when they triage cases based on financial exposure, strength of documentation, payer behavior, and whether the account could support a useful pattern argument against repeat underpayment.
That trade-off is easy to miss. A weak case with a large balance can consume more resources than it returns. A well-documented claim against a payer with a predictable low-pay pattern may justify fast escalation because the likely recovery and precedent value are higher.
The providers that perform well under the NSA usually build one closed-loop process. Intake captures the facts needed later. Billing flags underpayments early. The IDR team works from a standard evidence set. Finance tracks which payers underpay, which disputes settle, and which awards are slow to fund after decision.
Treat IDR as part of revenue recovery operations. The legal standard matters, but margin is usually protected or lost through documentation, timing, and claim-level discipline.
Creating Dispute-Ready Claims from the Start
Most air ambulance revenue problems that surface in negotiation or IDR were planted much earlier. The intake note was incomplete. The eligibility screen missed a plan detail. The chart proved the patient was sick but didn't fully explain why air transport was necessary at that moment, from that location, to that destination.
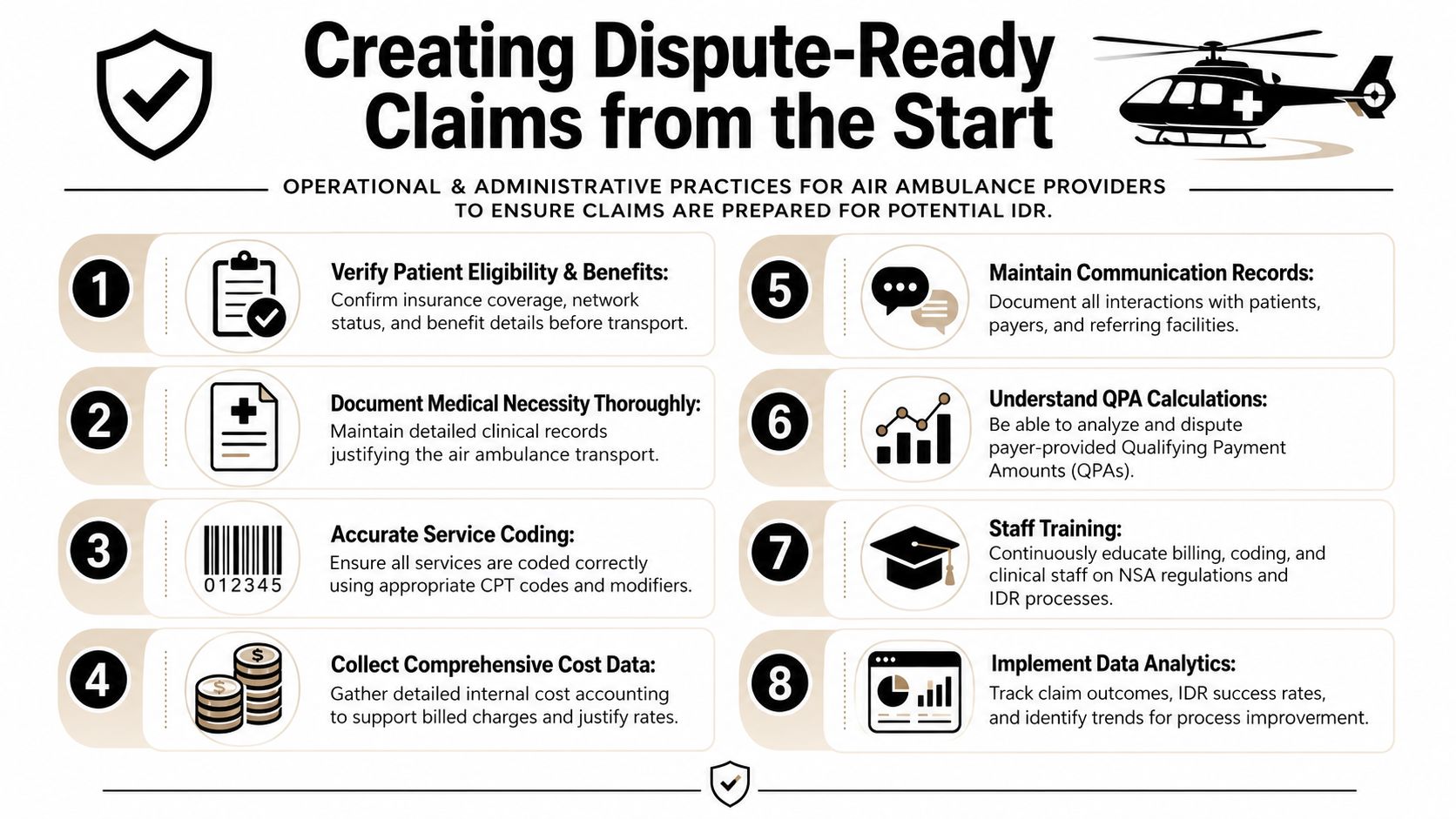
Under the NSA, air ambulance providers, insurers, and employer-based health plans must submit service and pricing data to CMS under section 106, creating a federal benchmark environment that raises the value of precise recordkeeping, as described in the CMS air ambulance data collection program. That makes sloppy documentation more expensive than it used to be.
What a dispute-ready claim looks like
A dispute-ready claim is not just a clean claim. It is a claim built so that, if challenged, the supporting record already exists.
That means your file should answer these questions without guesswork:
- Was the patient eligible and was coverage identified correctly?
- Does the chart show why air transport was clinically justified?
- Do coding and narratives match the actual service delivered?
- Can the team explain the payer response and rebut it quickly?
A lot of providers over-focus on the billed claim and under-focus on the evidence package behind it. Under the no surprises act air ambulance model, the evidence package often determines whether the claim holds value after the initial adjudication.
Documentation habits that pay off later
Some habits have outsized impact because they make downstream disputes easier to prove and faster to assemble.
- Lock in medical necessity language early: Generic urgency language is weak. The record should connect patient condition, risk of ground delay or limitation, and the receiving facility need.
- Preserve transport chronology: Time stamps, dispatch details, referring facility communications, and receiving acceptance records help defend the sequence of decision-making.
- Align clinical and billing records: If the nurse narrative, PCS-related support, and coded claim point in different directions, the payer will use the inconsistency.
- Track payer-facing correspondence: Every request, response, reconsideration, and negotiation message should be retained in a way that can be pulled into a dispute file.
One practical tool for operations teams is an RCM readiness checklist for NSA and IDR claims. Used properly, a checklist forces consistency across intake, chart completion, coding review, and dispute escalation.
Cost support is now part of the strategy
Operators sometimes hesitate to organize internal cost support because they assume the claim should stand on medical necessity alone. That's not enough in many disputes. Your internal accounting doesn't need to become the article of faith for the payer, but you do need organized support for the resources required to maintain aircraft readiness, specialized crews, and rapid-response capability.
Operational insight: The chart explains why the patient needed the flight. Your cost support helps explain why the payer's number doesn't reflect the service that was actually delivered.
This is also where integrated tools matter. Some providers manage the workflow in-house, some use outside counsel for selected disputes, and some use platforms such as RevGuard to connect eligibility, coding, denial management, and IDR execution in one operating model. The important point isn't the vendor choice. It's that the handoff gaps have to close.
Combating Common Payer Denials and Delays
A common air ambulance revenue problem starts the same way. The claim is submitted on time, the chart supports the flight, and payment still stalls because the payer changes the issue each time the file moves. First it is medical necessity. Then it is missing records. Then the plan cites coverage language or points to its payment as if the number settles the matter. Under the No Surprises Act, that sequence is not just administrative friction. It is a revenue tactic, and operators need to treat it that way.
Payers usually do not say the claim was reduced because the transport is high cost. They frame the dispute as process, documentation, or plan interpretation. For operators, the practical response is early classification. Identify whether the payer is contesting necessity, coverage, coding, or valuation before staff start sending records and drafting appeals. A mixed strategy wastes time and weakens the file.
The denials that keep showing up
Several denial patterns appear over and over in air ambulance accounts.
- Medical necessity challenge: The payer accepts that the transport occurred but argues ground transport could have handled the patient.
- Coverage denial: The plan says the service falls outside benefit terms, which is a different fight from an underpayment dispute.
- QPA anchoring: The payer treats its initial payment as presumptively reasonable and pushes the provider to disprove it.
- Documentation creep: The payer asks for more records in stages, extending account age and increasing deadline risk.
- Coding or bundling disputes: The payer reinterprets billed elements to reduce payable value.
Each category calls for a different workflow. A necessity denial belongs with a clinical rebuttal. A coverage denial needs plan language, authorization facts, and appeal positioning. A QPA-based underpayment requires preservation of the valuation dispute and a clean path to negotiation or IDR. Teams that study repeat payer behavior usually recover more because they stop treating every account as a custom project. For a practical reference, review common payor tactics in IDR and underpayment disputes.
How to answer them without wasting cycle time
The key is matching the response to the payer's actual position.
| Payer position | What it usually means | First provider move |
|---|---|---|
| “Air transport not medically necessary” | The payer sees room to argue for a lower-cost transport mode | Build a focused clinical response tied to acuity, time sensitivity, and destination capability |
| “Service not covered” | The dispute turns on plan adjudication, not just payment level | Separate the coverage appeal from any payment dispute immediately |
| “Payment based on QPA is appropriate” | The payer is anchoring low and forcing escalation | Review the rationale, preserve objections, and prepare for negotiation or IDR |
| “Need more documentation” | The payer may be testing file control or buying time | Send a complete, consistent response and log every request and deadline |
| “Code not payable as billed” | The payer is trying to reduce value through coding interpretation | Confirm coding support, compare billed services to the record, and rebut line by line if needed |
Operators lose margin. Staff often respond to a bad payment with activity instead of direction. More uploads, more emails, more reconsideration letters. None of that helps if the team has not identified the denial theory and assigned the right owner.
What weakens the account
Three habits show up in underperforming denial teams.
Sending every record without a stated position gives the payer more room to create side issues. The better approach is selective support tied to the reason for denial.
Arguing price when the payer is denying coverage misses the actual dispute. Coverage and valuation can overlap, but they should not be handled as if they are the same issue.
Letting the file drift is expensive. An air ambulance claim can look recoverable for weeks, then age past the point where the strongest appeal, negotiation, or IDR options are still available.
The most expensive denial is often the one that looked temporary, sat untouched, and aged past the point where the best procedural options were still available.
The operational trade-off is simple. A highly manual team may save money on the front end, but it usually gives that money back in missed deadlines, inconsistent rebuttals, and weak escalation discipline. Under the NSA, payer resistance is part of the reimbursement process for air ambulance providers. Revenue recovery depends on recognizing that reality early and managing denials as a coordinated RCM and dispute function, not a series of isolated follow-ups.
Conclusion Building a Proactive Revenue Protection Strategy
The no surprises act air ambulance environment rewards operators that stop treating reimbursement as a back-office clean-up function. Revenue protection now starts at first contact and runs through final payment. If dispatch, clinical staff, coders, billers, and dispute managers work in silos, the payer will find the seams.
The practical shift is straightforward. Build every claim as if it may need to survive scrutiny. That means stronger eligibility work, sharper medical necessity documentation, cleaner coding, disciplined correspondence tracking, and early recognition of whether the issue is coverage, valuation, or both.
The integrated model that holds up
A durable strategy usually has four traits:
- Shared ownership: Clinical teams understand what documentation supports payment, and billing teams understand what clinical facts matter most.
- Fast escalation rules: Staff know when to negotiate, when to appeal, and when to prepare for IDR.
- Evidence discipline: Records are organized for use, not just stored for compliance.
- Payer intelligence: The organization learns from repeat denial patterns instead of treating each account like a surprise.
In this context, many providers either regain control or keep bleeding value. A reactive shop fights one denial at a time. A proactive shop engineers fewer defects, better files, and stronger dispute outcomes across the portfolio.
What providers should take from the NSA
The statute protected many patients from balance billing for covered emergency air ambulance services. It also moved the hardest financial questions into the provider-payer channel. That's why the right response is not just compliance. It is operational design.
When an operator links front-end revenue cycle work with post-adjudication enforcement, the claim has a better chance of holding its value. When those functions stay disconnected, every low payment becomes a scramble.
Air ambulance providers don't need more abstract commentary about patient protections. They need a system that identifies revenue risk early, builds dispute-ready claims, and pushes recoverable underpayments through a disciplined negotiation and IDR process.
RevGuard helps providers connect front-end revenue cycle work with No Surprises Act dispute execution, including eligibility review, coding support, denial management, and IDR case development for air ambulance claims. If your team is dealing with recurring underpayments, delayed adjudication, or weak handoffs between billing and arbitration, you can review RevGuard's workflow at RevGuard.