In 2024, 36% of U.S. households had medical debt, and among people contacted about at least one bill, the average amount under collection was $7,931, according to a peer-reviewed analysis in PubMed Central on medical debt and collections. That changes how practice managers should think about collections. This isn't a back-office nuisance. It's a revenue-risk problem sitting in plain view.
Medical collections software matters because healthcare revenue no longer breaks cleanly into front-end intake, claim submission, payer follow-up, and patient billing. Every handoff creates leakage. A registration error can become a denial. A denial can become patient balance confusion. A poorly documented patient contact can become a complaint, a write-off, or an avoidable dispute.
The old model treated collections as the last stop. Send statements. Place reminder calls. Escalate aged balances. That model doesn't hold up when payer behavior is inconsistent, patients question bills more aggressively, and providers need cleaner documentation from the first touch through final payment. Modern medical collections software should protect revenue across the whole lifecycle, not just chase unpaid balances after the fact.
The New Reality of Healthcare Revenue
Most organizations still talk about collections as if the only question is how to recover more cash. In practice, the bigger question is how to stop revenue from leaking before an account ever reaches a collections queue.
A patient balance rarely starts as a simple self-pay obligation. It may begin with eligibility gaps, authorization defects, coding mismatches, underpaid claims, misapplied remits, or a patient who never should have been pushed into standard collections in the first place. If your software only starts working after a balance ages out, you're using it too late.
Revenue protection starts before collections
Medical collections software should sit inside a broader revenue protection strategy. It needs to inherit clean data from registration, claims, and remittance workflows. It also needs to return usable information to operators who manage denials, underpayments, payment plans, and disputes.
That distinction matters operationally:
- Administrative collections thinking focuses on sending notices and logging calls.
- Revenue protection thinking focuses on account validity, payer responsibility, patient affordability, and documentation quality.
- Dispute-ready thinking assumes every high-friction account may later need defensible records.
Practical rule: If staff members are manually reconciling balances across the practice management system, clearinghouse reports, and payer portals before they can even begin follow-up, the collections problem started upstream.
The most effective teams don't separate collections from the rest of revenue cycle management. They connect pre-service data quality, claim accuracy, adjudication history, patient communications, and escalation logic into one controlled workflow. That's what makes software useful. Not automation by itself, but automation tied to accountable process design.
What has changed for practice managers
Patients are more likely to question bills. Payers are more likely to delay, deny, or underpay. Staff turnover makes tribal knowledge less reliable. Compliance scrutiny has also widened the cost of sloppy outreach.
A modern platform has to do more than move balances through a queue. It has to help teams answer basic but high-value questions quickly:
- Is this balance correct
- Is the payer portion exhausted
- Does this patient qualify for financial assistance
- Has anyone documented the account well enough to defend the next step
- Should this account be resolved, appealed, written down, or collected
When software supports those decisions, collections becomes a controlled extension of RCM. When it doesn't, it becomes a cleanup crew for preventable mistakes.
Understanding Medical Collections Software Today
Medical collections software used to mean statement generation, aging reports, and basic remittance posting support. That definition is outdated. The category has expanded with the rest of healthcare billing infrastructure.
According to Meditab's overview of revenue cycle management, RCM tracks patient care episodes from registration and scheduling through final payment, and the surrounding U.S. medical billing services market included 1,364 businesses in 2024 and was projected to reach $4.8 billion in revenue by the end of 2024. That context explains why medical collections software now behaves less like a reminder tool and more like a post-adjudication control system.
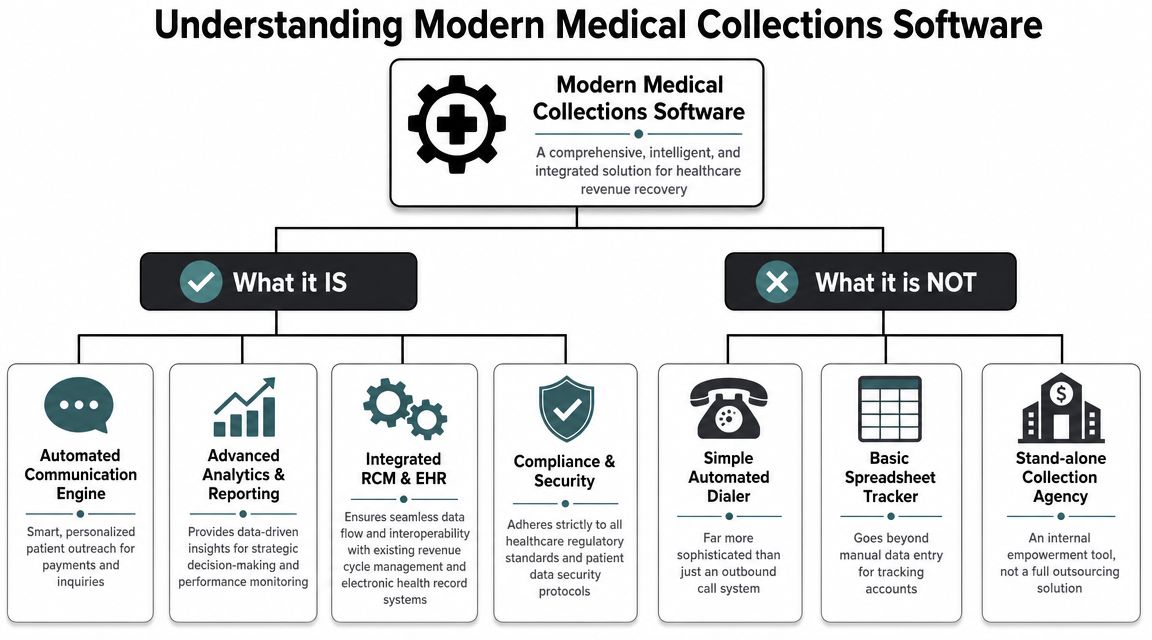
What it is and what it isn't
Think of modern medical collections software the way you'd think about a GPS versus a paper map. A paper map tells you where roads are. A GPS tells you where you are now, what changed, which route is blocked, and what to do next. Practices need the second version.
Basic accounting tools can record balances. They can't reliably orchestrate healthcare-specific collections logic across payer activity, patient outreach, and audit trails. A spreadsheet can list aged accounts. It can't decide whether a balance should be paused because an ERA posted incorrectly, a denial is still appealable, or the patient may qualify for assistance.
The practical definition that matters
For practice managers, the useful definition is simple. Medical collections software is the operating layer that manages unresolved reimbursement after billing begins. That includes patient balances, denial follow-up, communication history, payment arrangements, account segmentation, and escalation controls.
Strong systems usually support work such as:
- Queue management: Staff need prioritized worklists based on account status, not generic aging alone.
- Communication tracking: Every letter, call attempt, portal message, and payment promise should be visible in one record.
- Balance logic: The software should distinguish open patient responsibility from unresolved payer liability.
- Workflow control: Accounts should move through rules, not memory.
A collections platform should reduce ambiguity. If a collector has to ask three departments whether a balance is collectible, the software isn't doing enough.
Why this shift matters operationally
The organizations that get value from these platforms don't treat them as stand-alone call center tools. They use them to coordinate the messy middle between claim adjudication and true account resolution.
That means the software has to support two different realities at once. Some balances need straightforward patient payment workflows. Others need correction, appeal, refund review, charity-care screening, or legal and regulatory restraint. The platform has to help your staff tell the difference early.
A practice that buys software only for outbound reminders usually ends up disappointed. The tool may automate contact volume, but it won't fix account quality, payer handoff failures, or weak escalation rules. That's why implementation fails so often. The software isn't wrong. The operating model around it is too narrow.
Core Features Driving Revenue Recovery
The strongest medical collections software doesn't start with outbound collections. It starts with claim quality and payment integrity. If the claim enters the system with preventable defects, downstream collections becomes more expensive, slower, and harder to defend.
Elinext's review of medical billing software features identifies four functions that belong in a technically robust stack: claims scrubbing, eligibility verification, denial management, and remittance tracking. Those are not side modules. They are the controls that keep collections from becoming a rework department.
Upstream controls that prevent bad downstream balances
Here is what these features solve inside a practice:
- Claims scrubbing catches coding and formatting defects before submission. Without it, staff spend time working accounts that should have paid correctly the first time.
- Eligibility verification reduces the risk of sending patient statements based on incorrect coverage assumptions.
- Denial management gives staff a structured place to classify, route, and act on payer objections instead of letting denied claims drift into patient responsibility by default.
- Remittance tracking helps reconcile what was billed, what was allowed, what was paid, and what remains unresolved.
If a vendor markets itself as collections software but can't show these adjacent controls or integrate tightly with them, expect manual cleanup.
Features that help staff recover revenue, not just contact patients
Once account quality is under control, the next layer matters just as much. In day-to-day operations, I look for software that handles the following without forcing staff into side spreadsheets:
| Function | Why it matters |
|---|---|
| Work queues by account type | Staff need different playbooks for denials, underpayments, self-pay balances, and disputed accounts |
| Communication history | Supervisors need a complete record before escalation or write-off decisions |
| Payment plan management | Patients are more likely to resolve balances when terms are clear and documented |
| Statement and portal coordination | Mixed messages create duplicate calls and slow payment |
| Exception flags | Teams need to spot balances that should pause for review, correction, or assistance screening |
What works and what usually doesn't
What works is rule-based automation with human review at the right points. For example, the software can trigger outreach, suppress contacts while an appeal is active, and route disputed balances into a review queue. Staff then intervene where judgment matters.
What doesn't work is high-volume automation with weak account logic. If the system sends aggressive reminders on balances that are still tied to unresolved payer liability, you create avoidable complaints and damage trust with patients.
Field lesson: The best collections workflow is often the one that prevents the wrong account from being collected at all.
A useful platform reduces clicks, reduces duplicate review, and preserves a clean chronology. It should help your team answer, in one place, what happened, who touched the account, what the payer did, what the patient was told, and what should happen next.
Integrating with RCM and IDR Workflows
Standalone collections software is obsolete for any provider group dealing with denials, underpayments, and complex out-of-network reimbursement. If your collections platform can't connect to upstream RCM and downstream dispute workflows, it will miss the highest-value revenue problems.
The dispute-ready claim starts early
Practice managers often see collections as the final stage of the account. Under the No Surprises Act environment, that view is too narrow. By the time an underpayment or reimbursement dispute needs formal escalation, the quality of your earlier documentation determines the strength of your position.
A dispute-ready claim includes clean eligibility data, accurate coding, timely billing, traceable remittance activity, and a reliable communication log. It also includes evidence that your team handled the account consistently. That is why collections software has to do more than record promises to pay. It has to preserve a defensible timeline.
For organizations tightening payer follow-up, a structured healthcare denial management workflow often sits directly beside collections operations. The handoff matters. A denied or underpaid claim should not slip into patient responsibility just because one queue closes faster than another.
Where integration creates real value
Integrated systems support three things that fragmented stacks struggle to do:
- Carry forward account truth: Patient responsibility should reflect adjudicated reality, not whatever someone manually keyed after reading an EOB.
- Protect escalation paths: When an account moves from billing to collections to dispute review, documentation should move with it.
- Separate collectible from contestable balances: Some dollars belong in patient follow-up. Others belong in payer escalation.
This is especially important in specialty and emergency settings where reimbursement disputes are common. Teams need software that can pause, segment, and reroute accounts based on legal, contractual, and adjudication status.
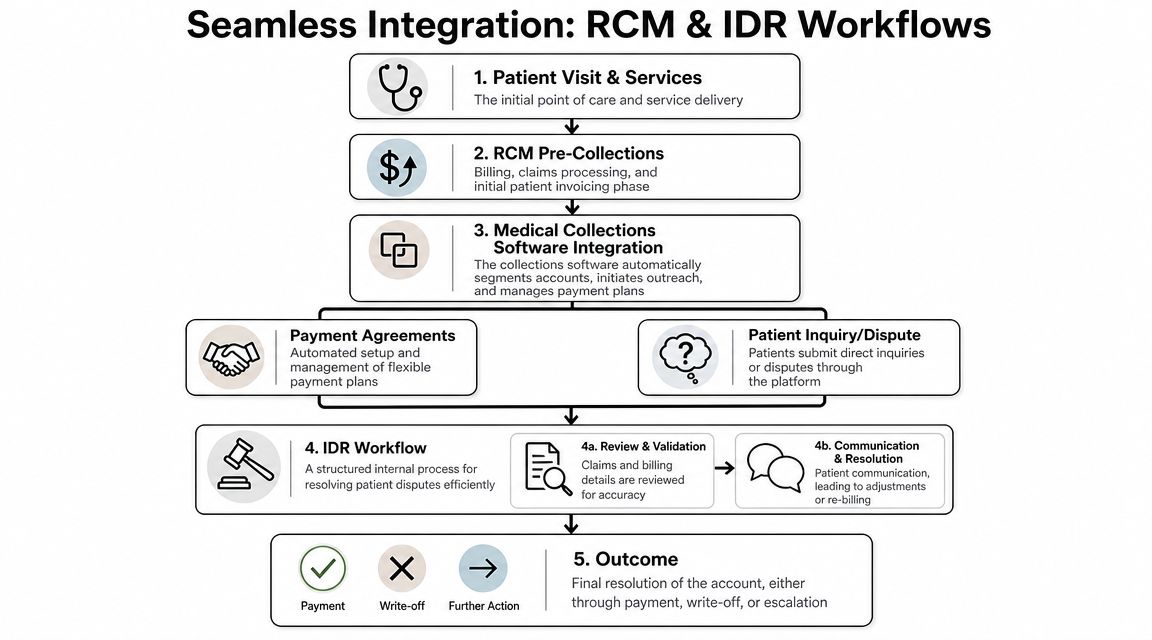
The practical operating model
A useful integrated workflow looks like this in practice:
- Front-end data enters cleanly. Eligibility and patient responsibility estimates are captured with enough accuracy to support later billing.
- Claims and remits sync into the account record. Staff can see what was billed, what was processed, and where exceptions remain.
- Patient outreach follows account logic. The system suppresses or changes outreach when disputes, denials, or corrections are active.
- Escalation remains evidence-based. If the account moves into payer dispute or arbitration-related support, the record is already organized.
What breaks this model is siloed ownership. Billing says the balance is patient responsibility. Collections says the payer issue is closed. Compliance says documentation is incomplete. Finance sees only aging. Integration fixes that by forcing one account history across functions.
A collections platform should never push revenue into the wrong bucket simply because it can't see what the denial team or reimbursement team is doing.
When a vendor can't explain how its platform supports payer underpayment workflows, dispute documentation, and traceable account transitions, it's not built for today's reimbursement environment.
Ensuring Compliance and Patient-Centricity
The old collections mindset asked one question: how do we get paid faster. The better question is whether the account should be pursued through standard collections at all.
That change isn't only about compassion. It's about operational accuracy, legal exposure, and bad debt control. Experian's patient collections guidance emphasizes patient financial segmentation, identifying uncollectable accounts, and using performance reporting to monitor self-pay vendors. In the same broader shift, Undue Medical Debt reports that it has abolished more than $10 billion in medical debt for 6.5 million families, reinforcing the move toward relief-oriented triage in some cases rather than recovery alone.
Compliance starts with account classification
Many compliance failures happen because teams apply the same workflow to every balance. That creates obvious problems. A patient who qualifies for assistance gets standard dunning notices. A disputed balance receives routine payment pressure. A payer-caused issue lands in external collections. None of that is defensible.
Modern software should help classify accounts before outreach intensifies. In practice, that means screening for hardship indicators, identifying unresolved billing issues, and routing certain balances into review instead of acceleration.
Organizations refining this process often pair software with specialized patient collections services for healthcare accounts when internal teams need more structured segmentation and oversight. The key isn't outsourcing by itself. The key is using a process that distinguishes inability to pay from unwillingness to pay.
What compliant, patient-centered workflows look like
Strong workflows usually include a mix of controls such as:
- Communication suppression rules for accounts under active dispute or correction
- Charity-care or financial assistance routing before aggressive self-pay escalation
- Documented consent and contact preferences so outreach doesn't drift into avoidable compliance risk
- Policy-based escalation rather than collector discretion alone
What doesn't work is treating compliance as a legal disclaimer at the bottom of a statement. Compliance has to live in the workflow rules, the queue logic, the scripts, and the audit trail.
Why patient-centric collections often outperform blunt tactics
A patient who believes the bill is wrong won't behave like a normal payor. More reminders won't solve that. A patient who can't pay won't become collectible because the cadence got louder. In both cases, aggressive automation can raise complaints while lowering trust.
Operational judgment: The highest-performing collections process is often the one that exits the wrong accounts quickly and preserves staff time for balances that are both valid and collectible.
Patient-centricity isn't softness. It's segmentation. It means matching the collection path to the account reality. Practices that do this well usually see cleaner handoffs, fewer internal disputes, and more consistent policy enforcement because staff aren't improvising account by account.
Measuring Success with the Right KPIs
Most practices still judge collections software by one visible number: cash collected. That's incomplete. If you collect dollars through heavy manual effort, poor account selection, or weak audit controls, the software may be underperforming even when receipts look acceptable.
Tratta's discussion of healthcare debt collection implementation points to an underserved need: true performance visibility. National hospital data shows wide variation in collections practices, which is why buyers need benchmarking, policy controls, and auditability, not just reminder automation.
The KPI set that matters most
For practice managers, a useful scorecard usually includes metrics such as:
- Cost to collect: Are you spending too much staff time and vendor expense to recover each dollar
- Days to resolution for patient balances: How long do valid balances stay open once they reach patient responsibility
- Bad debt ratio: Are more balances aging into write-off because routing and follow-up are weak
- First-pass resolution rate: How often does the account get resolved without repeated touches, rebilling, or internal escalation
- Dispute volume by root cause: Are patient disputes driven by confusion, coding, payer processing, or estimate gaps
These don't need to be exotic. They need to be reliable and reviewed consistently.
What to look for in software reporting
A reporting package is useful when it helps you manage behavior, not just admire dashboards. I want to see whether the system can break performance down by location, specialty, payer class, collector, and account type. If all the reporting does is summarize total balances and monthly collections, you still won't know where process failure lives.
A better analytics setup answers questions like:
| Question | Why it matters |
|---|---|
| Which balances should never have entered collections | Shows failure in upstream routing |
| Which payer outcomes create downstream patient confusion | Connects claims issues to self-pay friction |
| Which staff queues stall the longest | Exposes workflow bottlenecks |
| Which policies are producing avoidable complaints | Helps compliance and operations align |
Teams that need stronger visibility across reimbursement and collections often invest in dedicated healthcare business analytics support so finance, operations, and RCM leaders can work from the same definitions.
If a KPI can't change a workflow, it's probably a vanity metric.
The point of measurement isn't to prove that your collectors are busy. It's to prove that your revenue protection process is accurate, efficient, and controlled.
Your Vendor Selection Checklist
A software demo can hide a lot. Most vendors can show clean screens, automated reminders, and payment plan workflows. The harder question is whether the platform can function inside your actual revenue cycle, with your specialties, your payer mix, and your compliance posture.
Treat vendor selection like choosing a revenue partner, not buying a utility.
Questions that expose fit
Use this checklist during demos, reference calls, and contract review.
| Evaluation Criteria | What to Ask |
|---|---|
| Integration with practice systems | How does the platform exchange data with our PM system, EHR, clearinghouse, and payment tools? Which steps are real-time versus batch? |
| Balance accuracy controls | How does the system prevent unresolved payer liability from moving into patient collections? |
| Denial and underpayment visibility | Can staff see denial status, remittance activity, and patient outreach history in one account view? |
| Account segmentation | How are accounts classified for standard follow-up, dispute review, hardship screening, and write-off consideration? |
| Financial assistance routing | Can the workflow suppress outreach and route patients into charity-care or assistance review before escalation? |
| Communication controls | Can we customize letters, call rules, portal messaging, and outreach suppression by account condition and state requirements? |
| Audit trail | What exactly is time-stamped and preserved for compliance review or reimbursement disputes? |
| Reporting depth | Can reports be broken down by specialty, location, payer class, collector, and resolution path? |
| Specialty fit | What experience do you have with our specialty's billing and reimbursement patterns? |
| Escalation support | How does the platform support disputed accounts, payer underpayments, and downstream enforcement workflows? |
| Implementation model | Who maps workflows, tests logic, trains staff, and owns post-go-live optimization? |
| Governance | How are policy changes, rule updates, and user permissions managed and documented? |
Red flags to catch early
Watch for answers that sound polished but stay vague.
Be cautious if a vendor can't explain how it handles contested balances, can't show true queue logic, or treats compliance as a separate manual process. The same goes for platforms that rely heavily on CSV exports and side spreadsheets to manage exceptions. That's usually a sign the software won't hold up under real payer and patient complexity.
Also ask one blunt question: what types of accounts should never enter normal collections from this platform? A serious vendor will have a clear answer. A weak one will talk only about outreach cadence and payment conversion.
The right platform should help your staff decide what to collect, when to pause, when to escalate, and how to document every step. If it only helps you send more reminders, keep looking.
RevGuard offers specialty-specific RCM and IDR support for providers that need collections workflows connected to denial management, payer underpayment recovery, and dispute-ready documentation across the full revenue lifecycle.