
A patient hands your front desk a current insurance card. The visit happens. The claim goes out clean, at least on the surface. Then the remittance lands with an eligibility denial, or a benefit limitation nobody caught, or a network issue that turns a routine encounter into a payment fight.
That situation is common enough that many teams shrug and treat it as payer noise. That's a mistake. Medical eligibility verification is where revenue protection starts, and in a No Surprises Act environment, it's also where your advantage in disputes starts. If your staff verifies only that a policy appears active, you haven't verified enough. You have checked existence, not payment risk.
A strong front-end process does more than prevent avoidable denials. It creates a dated, documented record of what coverage looked like before service, what benefits were returned, what authorizations were required, what network status applied, and what the patient was told. That record matters when a payer changes its story after the claim is filed, and it matters even more when underpayment or out-of-network reimbursement disputes move into a formal escalation path.
Why Eligibility Verification Is Your First Line of Defense
The most expensive eligibility failures don't usually start with obviously bad data. They start with partial verification.
A scheduler confirms that coverage is active and moves on. Nobody checks the effective date against the date of service. Nobody confirms whether the rendering provider is in network under that specific product. Nobody reviews the referral rule, the authorization trigger, or the procedure exclusion. By the time billing sees the denial, the visit is over, the chart is closed, and staff are trying to reconstruct what should have been verified at intake.
A valid card is not a clean claim
An insurance card helps identify a plan. It doesn't prove that the patient is currently eligible for the exact service you're about to provide. It also doesn't prove that the benefit is available at your place of service, under your provider type, on that date, with that authorization status.
That distinction is where front-end discipline pays off. Eligibility work isn't clerical cleanup. It's a control point that protects reimbursement, supports point-of-service collections, and reduces downstream appeals. Teams that treat it as a checkbox usually end up building expensive rework into billing, follow-up, and denial management workflows.
Practical rule: If your verification note wouldn't help an appeals or arbitration team defend the claim later, it probably wasn't detailed enough.
Revenue protection starts before care
When eligibility is done correctly, three things happen early:
- Coverage is confirmed against the actual encounter. Not just the patient.
- Financial responsibility is clarified. Staff can collect copays, discuss deductibles, or route to counseling before service.
- Dispute evidence is created. The record shows what the payer or verification channel returned before treatment.
That last point gets missed in most conversations. In specialties that face aggressive payer behavior, the verification record often becomes the first contemporaneous evidence in a payment dispute. If the payer later argues that a service wasn't covered, required a referral, or fell under different benefit terms, your team needs more than a screenshot that says "active." You need timestamps, channel used, data returned, and staff actions taken.
The cost of getting this wrong
The financial impact isn't limited to one denied claim. A weak verification process causes a chain reaction: rework for registration, calls from patients who thought they were covered, rebilling, delayed cash, avoidable write-off pressure, and weaker footing when you're challenging underpayment.
In other words, eligibility isn't the first step because it's administrative. It's the first step because everything after it depends on whether you got the facts right.
The End-to-End Patient Eligibility Workflow
Think of eligibility as a financial pre-flight check. If the aircraft leaves the ground with the wrong inputs, the problem doesn't stay in scheduling. It follows the encounter all the way to billing and collections.
A reliable workflow has to be chronological, documented, and tied to the exact service date.
Start before the appointment
The highest-value work happens before the patient arrives. Industry guidance recommends collecting the insurance ID, group number, subscriber details, plan type, and effective date at least 48 hours before the visit, then confirming active coverage, copay, deductible, out-of-pocket limits, prior authorization requirements, and procedure-specific exclusions through payer portals, EDI, or IVR because those variables directly affect patient liability and authorization risk. Medusind's guidance on electronic benefit verification is useful on that point.
That timing matters because benefit rules are date-sensitive and service-specific. A patient can be active under one product and still not be covered for the scheduled procedure at your site of care. If your team waits until check-in, you've lost room to fix problems without rescheduling, self-pay conversion, or frantic same-day calls.
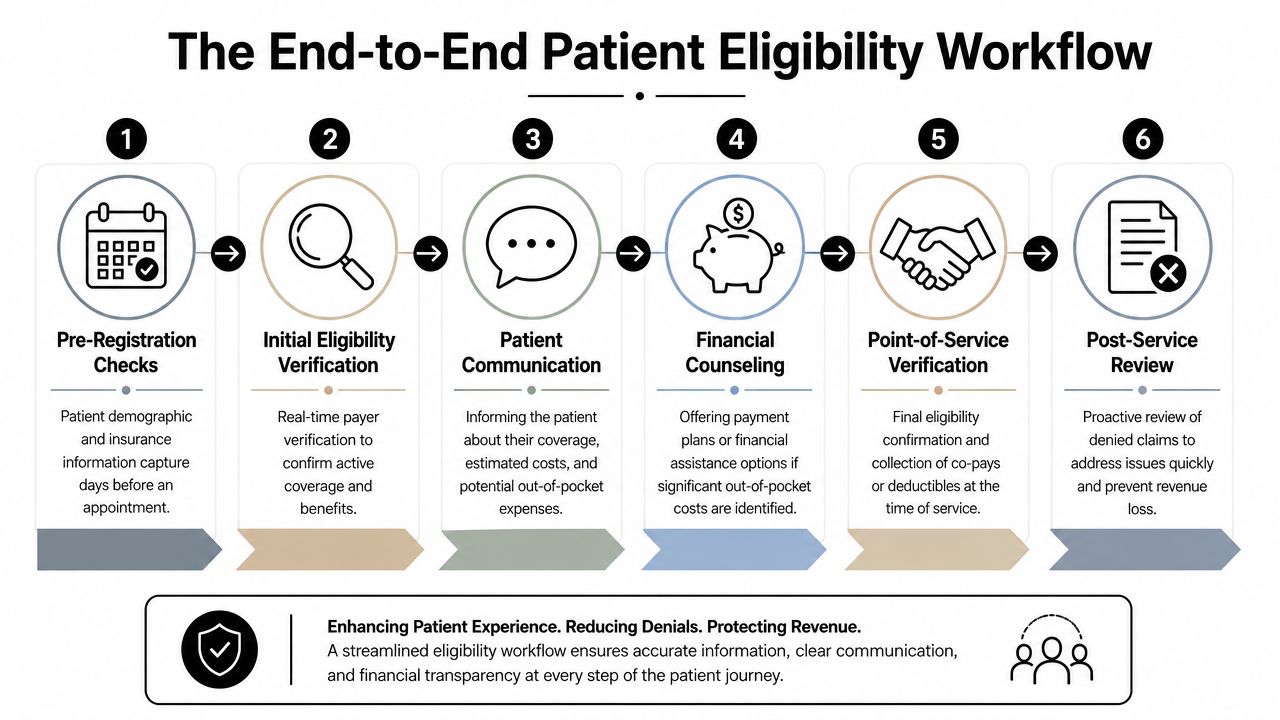
The six operational stages
Pre-registration intake
Gather full demographics and complete insurance details. Incomplete intake data creates weak verification, even if your technology is excellent.Initial eligibility check
Run the inquiry through your primary channel. Confirm that the plan is active and that the response matches the patient and subscriber relationship.Benefit validation
Go beyond status. Confirm cost share, service limitations, authorization rules, referral requirements, and network implications tied to the scheduled encounter.Patient communication
Tell the patient what was verified and what remains uncertain. If something requires follow-up, say so clearly.Day-of-service confirmation
Recheck when needed, especially for same-day scheduling, long-booked appointments, or plans known to change frequently.Post-service exception review
If the claim still denies on eligibility or benefits, compare adjudication against the original verification record immediately.
The cleanest claims usually come from boring workflows. The team followed the same sequence, documented the same fields, and escalated the same exceptions every time.
Why the workflow changed
A major shift came in January 2014, when Affordable Care Act-era Medicaid and CHIP rules moved states toward a more modernized, data-driven verification model. Medicaid says states must rely on available electronic data sources to confirm application information to the extent useful, and every state submitted a CMS Verification Plan. The policy also allows attestation for many eligibility factors without extra documentation, while requiring action when electronic data changes eligibility status. That framework reduced dependence on paper and helped set the stage for the current real-time verification environment RCM teams now work in, as outlined in Medicaid's eligibility verification policies.
The operational takeaway is simple. Verification is no longer a paper chase. It's a live workflow, and your process has to behave that way.
Essential Data Points and Verification Channels
Most front desks can verify something. Fewer verify the right things in the right channel for their volume.
That's where process maturity shows up. Strong teams use a checklist for the data points and a decision model for the channel.
What must be verified every time
At minimum, your staff should capture and validate:
- Patient and subscriber identity. Name, date of birth, subscriber relationship, member ID, and group number.
- Plan details. Product name, plan type, and effective date.
- Coverage status. Whether the policy is active for the intended date of service.
- Benefit details. Copay, deductible, out-of-pocket exposure, and any service-level limitations.
- Utilization controls. Prior authorization, referral rules, and procedure-specific exclusions.
- Network position. Whether the provider, facility, or both are treated as in network or out of network under that plan.
If your specialty bills professional and facility components separately, verify both implications. If your contracts vary by site or rendering entity, a generic "in network" note won't protect you later.
The channel matters as much as the checklist
Some practices still treat phone, portal, and EDI as interchangeable. They aren't. Each has a different labor profile, documentation burden, and fit by scale.
| Method | Speed | Labor Cost | Scalability | Best For |
|---|---|---|---|---|
| Phone | Slower and dependent on hold time | Highest manual effort | Limited | Low-volume practices, edge cases, payer exceptions |
| Payer portal | Moderate | Moderate | Better than phone, but staff-heavy at scale | Small to mid-sized practices with manageable payer mix |
| EDI or clearinghouse workflow | Faster in routine workflows | Lower per transaction once configured | Highest | High-volume groups, centralized teams, multi-site operations |
New York Medicaid's MEVS guide makes this trade-off unusually clear. It says the telephone method is recommended for providers with fewer than 50 transactions per month and is the most economical method, while ePACES requires a PC, internet access, and a valid ETIN, and X12 or clearinghouse methods require appropriate software and HIPAA transaction support. That means verification isn't just a compliance task. It's an operating-model decision shaped by transaction volume, staffing, and technical maturity, as described in the MEVS methods reference guide.
What works and what doesn't
Phone calls still have a place. They work when payer responses are incomplete, when the service is unusual, or when you need confirmation that isn't available electronically. But phone-only operations break down fast in specialty settings with heavy daily volume.
Portals are workable but inconsistent. Staff have to remember where each payer hides referral rules, accumulators, or product-specific exclusions. Portal-based verification can be accurate, but it often creates fragmented notes and uneven documentation.
EDI-based workflows scale best when the practice has enough volume to justify setup and disciplined exception handling. They also pair well with centralized teams and related upstream functions such as credentialing services for provider and payer alignment, because the value of a fast eligibility response drops if your enrollment and network data are wrong.
Choose the default channel for efficiency. Choose the backup channel for evidence.
Best Practices for a Bulletproof Verification Process
A bulletproof process isn't one that never fails. It's one that catches failures early, routes exceptions clearly, and leaves an audit trail that billing can use.
The easiest way to strengthen medical eligibility verification is to stop relying on memory. Build rules, scripts, and escalation paths that make good verification the default.

Non-negotiable rules
- Verify before the visit, not at the desk. The most useful verification work happens before the appointment because benefit variables change patient liability and authorization risk. Waiting until arrival turns a fixable issue into an operational disruption.
- Tie the check to the exact service. "Active coverage" alone isn't enough. Staff need to verify benefits and restrictions connected to the planned procedure and date of service.
- Re-verify when the booking window is long. Coverage can change between scheduling and treatment. Long lead times need a second check closer to the encounter.
- Create an exception lane. Front desk staff shouldn't improvise when data conflicts. They need a written path for escalation to authorization, billing, or financial counseling.
- Document what was returned, not what staff assumed. Notes should identify the channel used, timestamp, plan response, unresolved issues, and next action.
Train for judgment, not just data entry
Scripts help, but they don't replace judgment. A well-trained registrar knows when a response is incomplete, when the plan data doesn't fit the service, and when a generic portal result needs backup verification.
That means training should focus on patterns such as:
- Subscriber mismatch
- Termed coverage close to service date
- Out-of-network facility or rendering mismatch
- Authorization ambiguity
- Plan-specific exclusions that require billing review
Staff don't need to memorize every payer rule. They do need to recognize when the answer on the screen isn't safe enough to rely on.
Build written protocols for the common failure points
Most preventable denials come from a short list of front-end misses. Your protocol should spell out what happens when:
- The eligibility response shows active coverage but no clear benefits.
- The patient presents a card that doesn't match the payer response.
- The plan changes after pre-registration.
- The payer portal and EDI response conflict.
- The service requires authorization and the status is unclear.
One practical standard is to require a dated note plus attached evidence for any high-risk account. Screenshots, transaction responses, and call reference details give billing something concrete to work from later.
Technology and Workflow Integration for RCM
Eligibility becomes far more valuable when it isn't trapped inside one person's notes.
Modern web-based platforms can validate coverage specifics in seconds and update provider records through integration while reducing labor spent on calls and paperwork. In practice, that allows teams to check active coverage, benefits, referral rules, and out-of-network provisions before service instead of discovering issues after a denial. AIHCP's discussion of insurance verification in healthcare captures that operational shift well.

Integration is what turns speed into control
A fast eligibility response by itself doesn't protect revenue. It has to land in the workflow where schedulers, front desk staff, authorization teams, and billers all see the same version of the truth.
In a mature setup, the verification result feeds:
- Scheduling work queues
- Registration and check-in prompts
- Authorization follow-up
- Patient estimate and collection workflows
- Claim hold logic for unresolved front-end exceptions
That integrated record matters downstream. When a payer underpays or disputes network treatment, the organization can pull the original verification evidence quickly instead of rebuilding the file from scattered screenshots and staff memory.
Why this matters for IDR readiness
Under the No Surprises Act, payment disputes often turn on facts that front-end teams are in the best position to capture early. Network status, service classification, place of service, authorization posture, and benefit information can all affect how a payer frames reimbursement.
A dispute-ready verification process does three things well:
- Preserves evidence. Keep the original response, not just a summary note.
- Links front-end facts to the claim record. Billing and legal review shouldn't have to hunt across systems.
- Flags contradictions. If adjudication conflicts with verified data, staff can escalate faster.
Here, eligibility stops being a registration task and becomes part of an enforcement strategy. A dated verification record won't solve every underpayment dispute, but it can strengthen the factual backbone of the case.
For teams that want eligibility connected to later patient balance and payment workflows, platforms such as medical collections software can sit adjacent to the front-end process so unresolved balances follow a documented path rather than becoming disconnected collection problems. RevGuard also positions eligibility verification as part of a broader revenue-protection workflow that extends through final payment and dispute handling.
If your verification record can't travel with the claim, the organization loses leverage every time a payer changes the rationale later.
Key Metrics for Measuring Verification Performance
If you only track whether an eligibility check was completed, you're measuring activity, not reliability.
The core question is whether your verification process predicts payment correctly enough to prevent rework and support escalation when adjudication goes sideways.

Metrics that actually reveal process weakness
Focus on a short list of operational and financial indicators:
- Eligibility-related denial rate. Track denials tied to registration, coverage status, benefits, authorization linkage, or subscriber errors.
- Reverification rate for changed coverage. High rates can reveal payer mix issues or weak pre-service timing.
- Point-of-service collection performance. If verification is improving, front-end collections usually become more predictable.
- Manual touch rate by payer. This shows where your electronic channels are falling short.
- Turnaround time on verification exceptions. Slow exception handling often causes same-day problems that look like payer failures later.
Watch the gap between verification and adjudication
One of the most important patterns to monitor is the mismatch between what the eligibility inquiry returned and what the payer later did on the claim. CMS says the eligibility and benefit inquiry is meant to return real-time patient financial information such as deductibles, copays, and coinsurance, yet guidance still warns that an ID card doesn't guarantee active coverage and that eligibility should be checked before services are rendered. That exposes a persistent gap between transaction standards and operational reliability, especially for patients with changing coverage, as described by CMS in its eligibility and benefit inquiry overview.
That gap deserves its own dashboard view. If one payer repeatedly returns usable eligibility data and then adjudicates inconsistently, that is not just an internal process issue. It's a payer behavior issue.
Use metrics to decide where to invest
Metrics should drive action, not monthly reporting theater. If one specialty has heavy manual verification volume, redesign the workflow there first. If one payer creates repeated same-day eligibility reversals, require closer-to-service rechecks for that plan. If one clinic has weak documentation quality, retrain and audit notes.
Good measurement doesn't just reduce denials. It tells you where your process is thin and where the payer is unstable.
Specialty-Specific Notes and Compliance
A one-size-fits-all verification process usually fails in one of two places. It either slows down high-volume scheduled care, or it under-controls high-risk urgent care.
Dermatology, gastroenterology, orthopedics, and imaging centers usually benefit from disciplined pre-service workflows. They have scheduled encounters, procedure-driven benefit questions, and enough lead time to verify thoroughly, counsel patients, and fix authorization gaps before the visit. In those settings, standardization wins.
Air ambulance, emergency medicine, and other urgent services face a different reality. The patient may not be schedulable in the usual sense, and eligibility may need to be confirmed after stabilization or after the service starts. That doesn't make verification less important. It changes the sequence. These specialties need rapid post-event verification, strong documentation handoff, and precise records around network status and coverage facts that could matter later in payment disputes.
Compliance is tied to accuracy, not just completion
For No Surprises Act exposure, one of the most important front-end facts is whether the provider or facility is being treated as in network or out of network for the relevant service. If staff verify the wrong entity, or fail to distinguish between professional and facility status, the organization weakens its position before any payment discussion starts.
The right approach is specialty-specific, payer-aware, and written down. Practices that tailor verification rules to the actual encounter types they bill usually protect far more revenue than practices that chase uniformity for its own sake.
If your organization needs a tighter link between eligibility verification, denial prevention, and payment dispute readiness, RevGuard works across the full revenue lifecycle, from front-end eligibility and credentialing through collections and Independent Dispute Resolution under the No Surprises Act. That's useful for groups that don't just want cleaner intake, but a verification process that holds up when payers deny, downcode, or underpay.