
Most advice on medical billing compliance starts and ends with claim scrubbing, coder education, and policy binders. That advice is incomplete.
A claim can be technically clean, fully documented, correctly coded, and still get denied, downcoded, or repriced in a way that drains margin. That's the operational gap most specialty practices feel every day. Public guidance often treats compliance as a documentation and training problem, while the harder questions involve contract interpretation, payer-specific underpayment, and how to prove compliance when a payer challenges a claim that should have paid. One industry source notes that first-pass denials are common, citing 10 to 20% of claims denied on first submission in its discussion of non-compliance risk and payer-side disputes (UnisLink on hidden non-compliance risks).
That's why a modern compliance program has to do two jobs at once. It has to prevent preventable billing errors. And it has to create a record strong enough to support appeals, underpayment challenges, and No Surprises Act dispute work when the payer's behavior, not the provider's process, is indeed the problem.
Why Standard Medical Billing Compliance Is Not Enough
The standard playbook says this: train staff, scrub claims, submit on time, and audit charts. All of that matters. None of it is enough by itself.
A basic compliance program is built to answer one question. Did the practice follow the rules when it created and submitted the claim? In the current payer environment, specialty groups also need to answer a second question. Can you prove the claim should have been paid as billed when the payer denies, edits, or reprices it anyway?
Clean claim thinking is too narrow
Too many teams define medical billing compliance as error prevention only. That creates a blind spot. If your workflow stops at clean claim submission, you're compliant in a narrow sense, but you may still be exposed to revenue leakage from aggressive edits, inconsistent policy application, delayed payment, and post-adjudication underpayment.
That matters most in specialties where reimbursement turns on details such as modifier support, medical necessity narrative, prior authorization records, transport documentation, physician order language, or time-based elements in the chart. In those settings, the difference between a paid claim and a disputed claim often isn't whether a box was checked. It's whether the file contains a defensible story.
Practical rule: A compliant claim should also be a dispute-ready claim.
What actually protects revenue
The practices that hold up better under payer pressure do three things differently:
- They document for downstream review: They don't rely on the final claim form alone. They preserve the coding rationale, supporting records, and payer-facing evidence that may be needed later.
- They separate provider error from payer behavior: A denied claim isn't automatically a compliance failure. Teams need a way to classify whether the issue came from coding, documentation, eligibility, timeliness, contract interpretation, or payer adjudication.
- They treat denials as feedback: Repeated denials by payer, edit type, or service line reveal where compliance controls need to tighten and where enforcement needs to start.
Medical billing compliance should be viewed as revenue protection infrastructure. If it only helps you avoid obvious mistakes, you're leaving money exposed after submission.
The Legal and Financial Stakes of Non-Compliance
Compliance failures create two kinds of exposure. One comes from regulators. The other comes from ordinary payment operations that slowly weaken cash flow.
Regulatory risk is the one practice owners usually think about first. Billing for services that aren't supported, coding beyond what documentation can defend, weak supervision over charge capture, poor handling of protected health information, or sloppy vendor oversight can all trigger serious scrutiny. In plain terms, the law expects claims to be accurate, supported, timely, and handled through secure processes.
The financial side is easier to underestimate because it often looks like routine friction instead of obvious non-compliance. But the numbers are large enough to show that billing failures are not edge cases. One widely cited industry benchmark says about 30% of insurance claims are denied on first submission, and 32% of those denials are attributed to coding issues. The same source reports that in FY 2024, Medicare Fee-for-Service had an estimated 7.66% improper payment rate, equal to $31.70 billion, while Medicaid's 5.09% improper payment rate translated into $31.10 billion in federal funds (Aptarro medical billing statistics).

What the legal risk looks like in practice
A specialty practice owner doesn't need a law school summary. You need an operational reading of the rules:
- Claims must match the record: If documentation doesn't support the code, the claim is vulnerable.
- Financial relationships must be structured carefully: Referral and compensation arrangements can create billing exposure if they aren't reviewed properly.
- Patient financial protections matter: In out-of-network and emergency settings, newer reimbursement rules changed how some payment disputes work, especially for groups operating in high-acuity service lines. This is especially relevant for providers dealing with the No Surprises Act and air ambulance reimbursement disputes.
- PHI handling is part of compliance: Billing data security is not separate from billing compliance. It's one control environment.
Why owners should care even without an audit
Most compliance breakdowns don't begin with a dramatic event. They begin with repeated small failures:
| Risk area | What it looks like operationally | Why it matters |
|---|---|---|
| Coding support | The chart doesn't fully justify the billed service | Payment can be denied, reduced, or recouped |
| Submission discipline | Claims go out late or incomplete | Timely filing and avoidable denials hurt cash flow |
| Denial handling | Staff rebill without root-cause review | The same errors keep repeating |
| Security controls | Too many people access billing systems | PHI exposure risk rises |
Compliance isn't just about avoiding penalties. It's about preventing routine payment defects from turning into chronic revenue loss.
Owners who treat compliance as a legal checkbox usually find out too late that they were really managing a margin problem.
The 7 Core Components of a Modern Compliance Program
A modern medical billing compliance program should do more than prevent bad claims from leaving the building. It should also leave the practice with records, logic, and process discipline strong enough to defend payment later. That is the part many owners miss. The same controls that reduce denials on the front end also give you a stronger file when a payer downcodes, recoups, or forces a dispute.
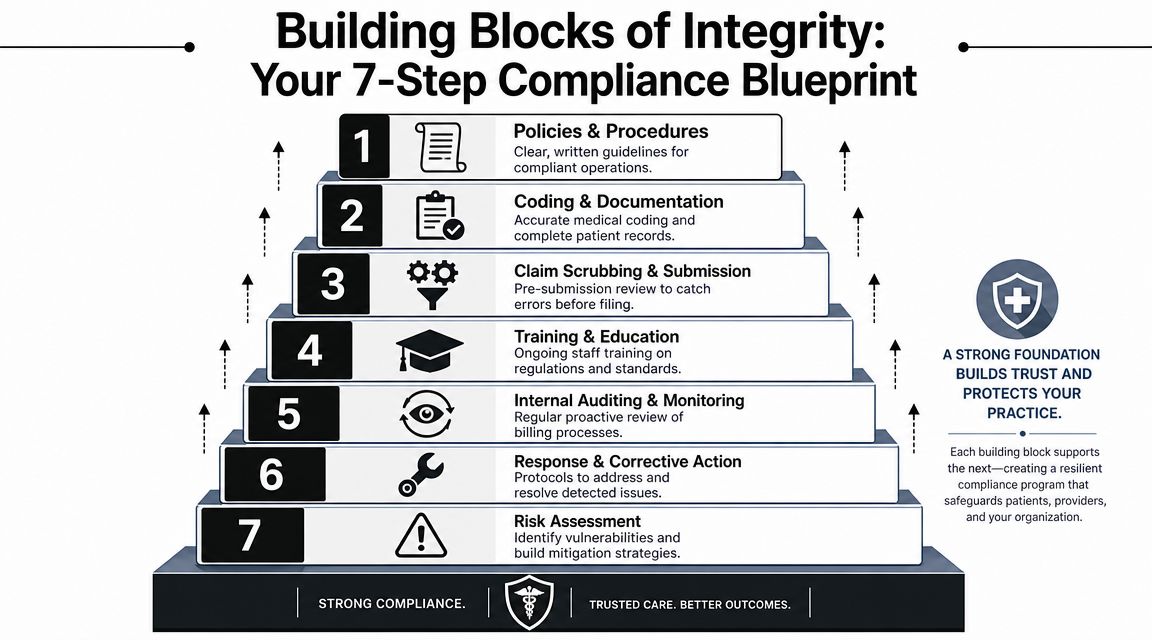
Policies and security controls
Written policies need to match actual billing operations. Template language pulled from a consultant binder will not help if your staff follows a different workflow. Policies should assign coding authority, define documentation standards, set claim correction rules, address credit balances and refunds, establish denial escalation, and spell out what outside vendors can and cannot do with your data.
Security controls belong in the same framework because billing compliance and PHI protection sit in one operational system. Basic controls include encryption for PHI at rest and in transit, multi-factor authentication, role-based access, audit logs, routine risk reviews, and patch management for systems that handle claim submission and remittance data (Zmed Solutions on billing security controls).
Coding and documentation integrity
This marks the beginning of payment defense.
Code selection has to match the chart, but that standard is too low for many specialty practices. The stronger test is whether an outside reviewer can follow the medical necessity, modifier logic, and service distinction without filling in the gaps from memory or clinical intuition. If the answer is no, the claim may pay today and fail later in audit, appeal, or dispute review.
For specialty groups, I would pressure-test three points:
- Does the documentation explain modifier use in plain, reviewable terms?
- Does the record show why the service was necessary at that time, in that setting?
- Would the file still make sense six months later to a payer reviewer who never saw the patient?
Claim scrubbing and submission discipline
Scrubbers help enforce consistency. They do not cure weak source documentation or missing payer logic.
Strong submission discipline usually includes pre-bill review for high-risk claims, filing deadline controls, payer-specific edit rules, and a defined process for holding claims that need clarification before submission. That last point matters more than many practices admit. Sending a questionable claim to “see if it pays” often creates rework, appeal cost, and a weaker record than pausing for one clean correction upstream.
A clean claim process should produce a bill you can defend, not just a bill that passes an edit.
Training and escalation
Annual compliance training checks a box. It rarely changes claim outcomes by itself.
Training should be short, recurring, and tied to real error patterns inside the practice. If a payer keeps denying a modifier, disputing medical necessity language, or reducing a recurring procedure code, the people who register, code, bill, and document need examples from those exact claims. General reminders are easy to ignore. Claim-specific teaching changes behavior.
Escalation rules matter just as much. Staff need to know when to stop routine rework and move the issue to physician clarification, contract review, legal review, or formal appeal. Without that handoff point, teams waste time rebilling claims that were never going to pay correctly without a stronger argument.
Auditing and monitoring
Auditing works when it creates feedback, not when it produces a quarterly spreadsheet no one uses. The best programs sample claims by risk, compare billed services to chart support, track denial causes, verify correction of repeat issues, and document who owns each fix.
Closed-loop monitoring is the goal. An issue found in audit should change edits, training, documentation prompts, or payer follow-up. The Medical Group Management Association describes compliance oversight in similar operational terms, with monitoring, auditing, reporting channels, and corrective action built into day-to-day practice management (MGMA on compliance program guidance).
Denial intelligence and corrective action
This component separates a defensive compliance program from one that protects revenue.
Denials should be classified by cause, not dumped into one work queue. Coding errors, missing documentation, eligibility failures, prior authorization problems, timely filing misses, contract underpayments, and payer repricing require different responses. If your team treats them the same way, root causes stay hidden and payer behavior goes unchallenged.
This is also where the link between compliance and revenue enforcement becomes obvious. A specialty practice that cannot show clean intake, defensible coding, and clear documentation will struggle to win an appeal or support a payment dispute. A practice with those controls in place has a stronger record for arguing that the billed service was proper and the payer's reduction was not.
Risk assessment
Risk assessment should direct attention and staffing to the claims that can hurt you most or pay you back the most if handled well. Review exposure by specialty, payer, place of service, procedure family, modifier use, denial trend, and claim value.
Every claim does not need the same level of review. A high-acuity out-of-network claim with complicated medical necessity issues deserves more scrutiny than a routine repeat service with stable payer rules. Good compliance design respects that trade-off. It protects staff time while putting tighter controls around the claims that carry the highest audit risk, recoupment risk, or dispute value.
Common Compliance Failures and Specialty-Specific Pitfalls
Most compliance failures don't begin as fraud. They begin as shortcuts, assumptions, and specialty workflows that were never translated into billing language.
An orthopedic group may have excellent operative documentation and still lose payment because the modifier logic isn't explicit enough for the payer's edit system. An anesthesia group may chart thoroughly but leave ambiguity around the separate nature of a service. An air ambulance provider may have strong clinical urgency in the record but weak billing support for why the transport met payer scrutiny. In each case, the care may have been appropriate. The billing file still isn't strong enough.
Where specialty practices get exposed
The most common trouble spots tend to look like this:
- Modifier overconfidence: Teams use modifiers such as -25 or -59 because the service feels distinct, but the chart doesn't state the distinction in a way an auditor or payer reviewer can follow.
- Medical necessity that lives in the clinician's head: The provider knows why a service was necessary. The note doesn't make that logic visible.
- Bundling mistakes: Charges are entered as separate payable services even when coding rules or payer edits treat them as packaged.
- Incident-to misunderstandings: Shared assumptions about supervision and service setup can drift away from what billing rules require.
- Template-driven records: Notes become too standardized and stop showing the facts that justify the billed level or service relationship.
What this looks like in real operations
A multispecialty ASC can have a strong front-end team and still create compliance exposure downstream. Scheduling confirms insurance. Clinical staff complete the chart. Coding goes out on time. Then denials pile up around repeat service combinations because nobody owns payer-specific edit review.
A hospital-based specialty group can have the opposite problem. The claim is coded correctly, but the payer reduces or downcodes after adjudication. Staff treat it like routine underpayment and rebill or appeal generically, even though the stronger route would be to preserve the exact clinical and billing evidence needed for a formal payment dispute.
The biggest compliance mistakes are often classification mistakes. Teams label a payer issue as a coding issue, or a documentation issue as a denial management issue, and then work the claim through the wrong channel.
A simple way to test for hidden risk
Ask your billing lead and your coding lead the same question about a recent denied claim: why was this denied? If you get two different answers, your compliance program probably has a handoff problem.
Use that test especially in specialties with frequent modifiers, split billing responsibilities, emergency services, transports, or high-value outpatient procedures. Those are the areas where a technically compliant process can still produce weak claims if teams don't share the same standard of proof.
An Audit-Ready Checklist and Key Performance Indicators
An audit-ready compliance program should do more than prove you tried to follow the rules. It should show, claim by claim, whether your process is preventing avoidable denials, preserving evidence, and identifying payer behavior that belongs in an appeal or payment dispute.
That requires a control structure people can use. Standardized pre-bill checks, targeted chart sampling, root-cause denial review, and documented corrective action give leadership a way to see where claims are breaking and whether the failure starts inside the practice or after the claim leaves it. If you need an outside read on that process, coding, auditing, and compliance support can help test whether internal workflows match what auditors and payers will expect.
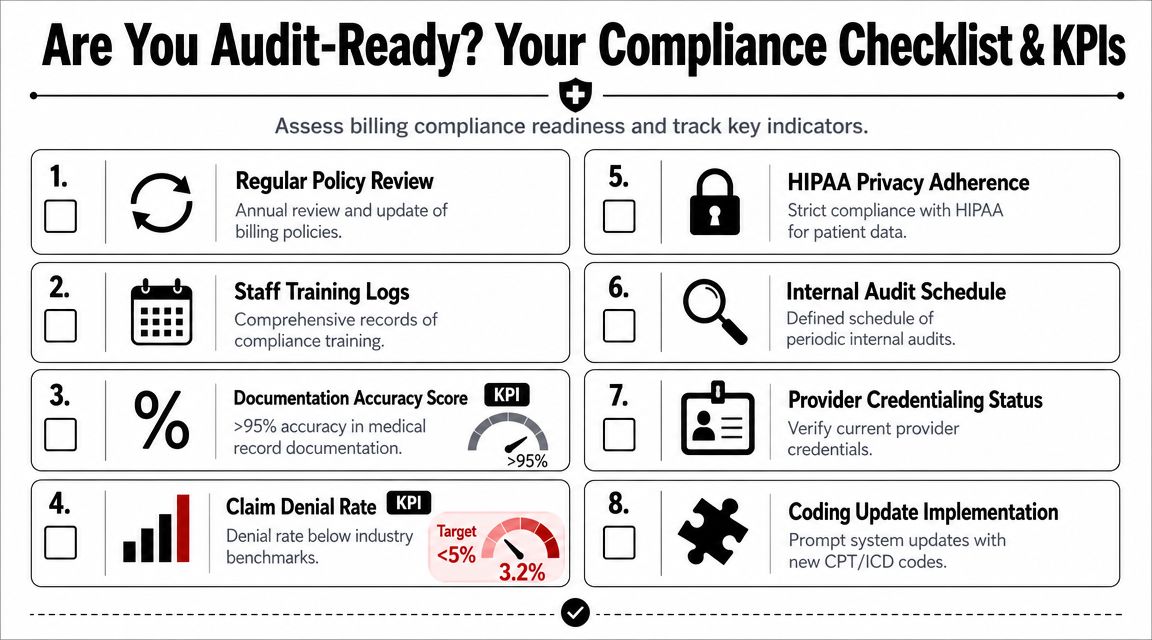
Audit-ready checklist
Use this checklist the same way an experienced revenue cycle leader would. Review it against actual claims, not policy binders.
- Policies match live operations: Billing, coding, refund, security, vendor oversight, and appeal policies reflect how staff work today, including specialty-specific exceptions.
- Training follows real error patterns: Education is role-based and tied to recent denials, audit findings, payer edits, and documentation failures.
- High-risk claims have a second review path: Modifier-heavy, high-dollar, repeated-procedure, and specialty-sensitive encounters get extra scrutiny before submission.
- Documentation can defend the claim later: The record supports medical necessity, code selection, setting, service distinction, and any facts a payer may challenge after adjudication.
- Pre-submission edits are configured by payer: Timely filing, authorization, eligibility, place-of-service, NCCI, modifier use, and contract-specific requirements are checked before release.
- Denials are classified by root cause: Staff separate registration, coding, documentation, and authorization defects from payer downcoding, bundling, repricing, or medical necessity disputes.
- Corrective action has an owner and a deadline: Repeat issues trigger policy updates, focused retraining, workflow changes, or escalation to leadership.
- Access and audit controls are reviewed: User permissions, change logs, vendor activity, and audit trails are monitored and documented.
The KPIs that matter
A useful compliance dashboard answers two questions. Are controls preventing bad claims, and are payers creating payment friction after clean claims go out?
| KPI | What to watch for | Why it matters |
|---|---|---|
| Clean claim rate | Claims accepted without preventable edits, rework, or missing information | Shows whether front-end, coding, and charge capture controls are working |
| Denial rate by root cause | Trends in eligibility, authorization, coding, documentation, filing, and payer processing | Separates internal defects from payer conduct |
| Underpayment variance by payer | Payment differences against contracted or expected reimbursement | Helps identify repricing patterns that should not be treated as routine denials |
| First-pass paid rate | Claims paid correctly on initial adjudication | Tests whether clean claims are also payment-ready claims |
| Appeal or dispute win rate | Which issues reverse, and which payers reverse them | Shows where preserved documentation is strong enough to recover revenue |
| Audit findings by category | Repeat errors in coding, documentation, modifier use, and policy adherence | Points training and monitoring to the highest-yield fixes |
| Time to corrective action closure | How long known issues stay open after identification | Measures whether the compliance program changes behavior or just records defects |
One management habit makes these metrics more useful. Review them with billing, coding, compliance, and a clinical leader at the same table.
That meeting changes the conversation. Clean claim rate may look fine while underpayment variance climbs. Audit findings may fall while payer bundling disputes rise. A practice that tracks both sides of the claim can spot the difference between a compliance failure and a revenue-enforcement opportunity, which is exactly what an audit-ready program should do.
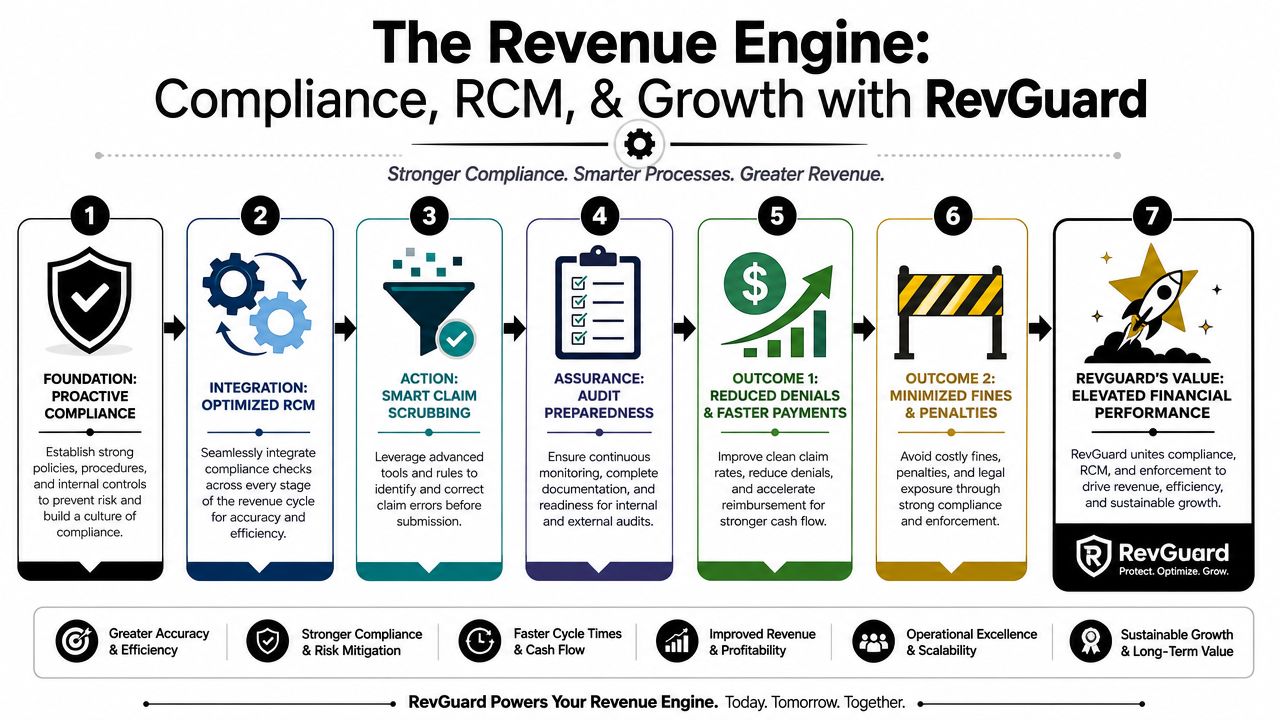
Beyond Clean Claims How Integrated RCM and Enforcement Drive Revenue
A clean claim is the starting line, not the finish line.
That's the part most medical billing compliance content misses. Newer reimbursement and enforcement conditions, especially in the No Surprises Act and IDR environment, raise practical questions that many articles don't answer, such as what evidence should be preserved for dispute-ready claims and how compliance programs should adapt when payers use more automated edits (MedUSA RCM on evolving compliance pressures).
Compliance should create evidence
An integrated revenue cycle takes each upstream step and asks a downstream question.
Eligibility verification is not just about confirming coverage. It creates the intake record that may matter later if the payer disputes the setting, plan status, or authorization pathway. Coding isn't just about selecting the right CPT or HCPCS code. It creates the clinical and technical rationale that may later support an appeal, underpayment challenge, or formal dispute. Payment posting isn't just bookkeeping. It reveals whether the payer honored the expected reimbursement logic.
That means the best compliance systems preserve more than the final claim:
- Supporting records: Notes, orders, transport details, and related documentation
- Coding rationale: Why a code set or modifier combination was selected
- Payer communication trail: Requests, responses, edits, and adjudication details
- Contract and rule context: The payment framework that should apply
What changes under payer pressure
When payers use more edits and automated repricing, a provider needs more than a correction workflow. You need an enforcement workflow.
For some claims, the correct response is rework. For others, it's a focused appeal. For others still, the issue belongs in a broader denial and dispute strategy. That's where integrated denial management matters. Teams that combine compliance review with healthcare denial management workflows are better positioned to distinguish ordinary defects from systemic underpayment patterns.
If your compliance process ends when the claim leaves the door, the payer controls the rest of the story.
The offensive model
This is the shift specialty groups should make. Don't build medical billing compliance only to avoid penalties. Build it so every claim file can support payment enforcement when necessary.
That approach changes how you value upstream work. Strong documentation, payer-specific billing logic, disciplined coding review, and clean audit trails don't just reduce denials. They enhance their position in disputes, especially in service lines where reimbursement is frequently contested and claims may need a more formal evidentiary path.
RevGuard is one example of this integrated model. It combines specialty-focused RCM work with No Surprises Act IDR enforcement so the same upstream billing process that creates clean claims also creates dispute-ready records for underpayment recovery. That linkage is where many practices still have a gap.
Putting It All Together Your Next Steps
Medical billing compliance works best when you stop treating it like a defensive checklist. It's an operating system for accurate billing, secure data handling, denial intelligence, and payment enforcement.
For specialty practices, the practical shift is simple. Don't ask only whether the claim is correct. Ask whether the claim file is strong enough to survive scrutiny from coders, auditors, payer reviewers, and dispute entities. That's what protects revenue in the current environment.
Three next steps usually make the biggest difference.
Start with a focused internal review
Pull a sample of recent denied, downcoded, and underpaid claims from one specialty line. Review them for coding support, documentation quality, timeliness, modifier logic, and payer response pattern. You're looking for classification mistakes as much as coding mistakes.
Rebuild your denial categories
If your denial buckets are broad, fix that now. Separate coding defects from documentation gaps, front-end errors, contract issues, and payer-side repricing. Until you do that, your team will keep applying the wrong remedy to the wrong problem.
Test whether your claims are dispute-ready
Choose a handful of high-value claims and ask whether you could assemble a persuasive payment file from what is already stored. If the answer is no, your compliance program is still built for submission, not enforcement.
A practice that can create clean claims and defend rightful reimbursement is in a much stronger position than one that only does the first half well.
If your team needs help connecting compliance, specialty RCM, and payment enforcement, RevGuard works with provider groups to build clean, dispute-ready claims across the revenue cycle and support recovery when payers deny, downcode, or underpay.