
A patient calls your billing office after a procedure and says the final bill is nowhere near what your scheduler mentioned on the phone. A week later, your practice gets a formal dispute notice. Suddenly, that casual estimate, the undocumented discount, and the patchwork billing process you've lived with for years stop looking harmless.
That's where a lot of specialty practices are right now. They still treat self-pay as an exception workflow. Front desk staff quote rough numbers. Clinical teams add services without tightening financial communication. Billing posts charges after the fact and hopes the patient understands. That model is over.
Introduction The New Reality of Self-Pay Billing
If you're leading revenue cycle for a specialty practice, you already know the pressure points. Patients are asking for prices before they commit. Staff want simple answers. Providers want scheduling to move faster. Meanwhile, every sloppy handoff between scheduling, coding, and billing creates exposure.
The old cash-pay mindset was informal by design. Quote a number, collect what you can, fix it later if needed. That doesn't work anymore. Self-pay billing now sits inside a regulated framework, and the risk isn't abstract. You can lose revenue, trigger disputes, spend staff time defending avoidable variances, and damage patient trust all from one encounter.
Why informal pricing fails
A verbal quote isn't a control. It's a liability.
When staff use “about,” “roughly,” or “usually” without a documented estimate tied to actual services, your practice creates a gap between expectation and bill. That gap is where complaints start. It's also where your collections rate weakens, because patients pay faster when the amount feels predictable and justified.
The deeper problem is operational. Most self-pay failures don't come from bad intent. They come from disconnected systems:
- Scheduling identifies the patient incorrectly
- Coding doesn't finalize expected services early enough
- The estimate excludes supplies, facility components, or professional components
- No one captures proof that the patient received the estimate
- Billing can't explain why the final amount changed
That's not just messy. It's expensive.
Practical rule: If your self-pay process depends on staff memory, side conversations, or manual exceptions, it isn't defensible.
What a bulletproof process actually does
A strong self-pay workflow protects both compliance and cash flow. It gives your staff a standard fee schedule, your patients a clear written estimate, and your billing team the documentation to support the final charge. It also forces discipline upstream. That's good for revenue.
Here's the standard I recommend:
| Process area | Weak practice | Defensible practice |
|---|---|---|
| Price communication | Verbal range | Written estimate tied to expected services |
| Fee setting | Chargemaster or ad hoc discounts | Approved self-pay schedule |
| Documentation | Scattered notes | Centralized audit trail |
| Collections | Bill after service and react | Pre-service expectation setting |
| Variance handling | “That's just how it coded” | Documented clinical and financial rationale |
The rules for charging self-pay patients are no longer something you hand to compliance and forget. They belong inside scheduling logic, charge capture, estimate generation, payment policy, and collections behavior. That's how you reduce disputes and protect margin.
The Legal Framework for Self-Pay Billing
A scheduler books an uninsured patient for a high-value specialty visit. The front desk gives a verbal price range. The physician adds imaging, supplies, or a second procedure on the day of service. Thirty days later, the patient gets a bill far above what they expected and files a dispute. At that point, your problem is no longer patient communication. It is a failed revenue cycle control.
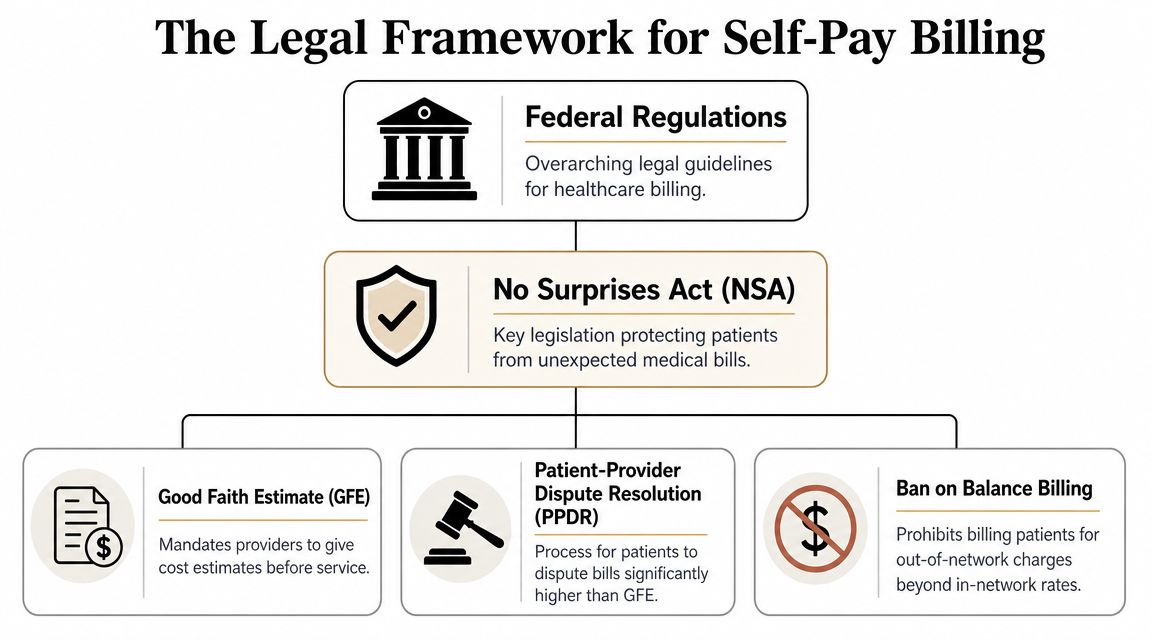
The legal baseline changed when the No Surprises Act Good Faith Estimate rules took effect on January 1, 2022. Under those rules, uninsured or self-pay patients must receive a written estimate of expected charges before care is provided, and the patient-provider dispute resolution process can be triggered when the bill is at least $400 above the estimate, according to this overview of the No Surprises Act self-pay requirements.
That rule changes how a specialty practice should build its workflow. A Good Faith Estimate is a financial document tied to identifiable services, expected charges, and a delivery record your team can produce later. If you treat it like a courtesy handout, you create preventable variance risk.
Here is the operational point many articles miss. The law does not sit off to the side. It dictates front-end decisions in scheduling, registration, charge routing, estimate generation, and final bill review. If those steps are disconnected, your practice will issue estimates that cannot survive contact with the actual claim or statement.
What the law requires your workflow to do
For specialty groups, the legal framework translates into three concrete controls:
- Identify the patient correctly at intake. Your staff needs a consistent method to flag uninsured and self-pay accounts before clinical services are scheduled or modified.
- Produce and deliver a written estimate on time. That means your system must pull the expected CPTs, professional components, and any known related charges into a document the patient can receive and your team can later retrieve.
- Control variance between the estimate and the final bill. If the service changes, your documentation needs to show why. If the bill changes, your revenue cycle team needs support that will hold up under outside review.
Those are legal duties, but they are also revenue protection controls.
The dispute process matters for that reason. Once a patient challenges a bill that materially exceeds the estimate, your practice may have to justify the difference to an independent reviewer. Billing staff cannot fix that after the fact with a vague note or a retroactive explanation.
Your estimate process should answer one question before service begins: if this bill is disputed later, can we show exactly what we expected to do, what we told the patient, and why the final charge changed?
Specialty practices should also understand that surprise billing enforcement does not exist in a vacuum. Related payment rules in other service lines show the same pattern: documentation, notice, and defensible charge logic determine who wins disputes. This overview of No Surprises Act rules for air ambulance reimbursement is a useful example of how regulators connect payment expectations to documentation standards.
The core takeaway for specialty groups
The legal standard is straightforward. Identify the right patient. Issue the right written estimate. Bill in a way that matches what you estimated or document the reason it did not.
Practices get exposed when they treat self-pay compliance as a billing-office problem. It starts earlier, at scheduling and registration, and it ends only when the final statement can be matched back to the original estimate and the clinical record.
Establishing a Defensible Self-Pay Fee Schedule
Most self-pay pricing problems begin with one bad decision. The practice uses its full chargemaster and calls it a self-pay rate. That's lazy, and it's risky.
A defensible fee schedule has to be grounded in what your practice accepts in the market, not what your legacy charge file says on paper. If you charge uninsured patients at inflated gross rates while accepting materially lower contracted rates from payers, you're inviting fairness complaints and scrutiny.
Stop using the chargemaster as your self-pay strategy
Your chargemaster might still serve an internal purpose. It should not serve as your public self-pay pricing philosophy.
A widely cited compliance benchmark is that self-pay charges should generally not exceed 1.5 times the provider's median contracted insurance rate for the same service, according to this self-pay pricing guidance. In practical terms, that same guidance explains that if a procedure is typically reimbursed at $1,000 by contracted insurers, self-pay pricing above about $1,500 can create legal and fairness concerns.
That benchmark gives you a workable guardrail. Use it.
Build your fee schedule from actual reimbursement data
I'd structure a specialty practice self-pay schedule around a documented review of contracted rates by CPT or service bundle. Then set approved self-pay amounts with leadership signoff and version control.
Use this framework:
- Start with median contracted reimbursement for the same service across your active payer mix.
- Set a clear self-pay amount that your staff can quote without improvising.
- Apply the same methodology consistently across the specialty, not case by case.
- Review high-variance codes first, especially procedures, add-on services, supplies, and imaging components.
- Create bundle logic where appropriate so the patient sees a realistic episode price instead of fragmented line items.
Put the discount policy in writing
Random discounts are one of the fastest ways to undermine your own defense.
If one patient gets a lower rate because they asked harder, and another gets a higher rate because the scheduler was rushed, your process isn't fair and it isn't controllable. Every self-pay reduction, prompt-pay option, or financial hardship adjustment should flow from a written policy approved by leadership.
A solid policy should answer:
| Policy element | What it should define |
|---|---|
| Base pricing method | How the self-pay rate is derived |
| Discount types | Prompt-pay, package pricing, hardship, or other approved categories |
| Approval rules | Who can apply adjustments and when |
| Documentation | What must be recorded in the account |
| Patient communication | How the amount is explained in writing |
Don't let staff “work something out” with a patient unless your policy already tells them exactly what that means.
Transparency is part of pricing now
The same self-pay pricing guidance notes that hospitals must publish standard charges, including self-pay rate information, under the Hospital Price Transparency Rule, reinforcing that self-pay pricing is part of a formal public disclosure regime rather than a private internal policy. Even if your entity type has different obligations than a hospital, the operational lesson is obvious. Hidden pricing is a bad strategy.
The best self-pay fee schedules are boring. They're approved, repeatable, documented, and easy for staff to use. That's what makes them defensible.
Operationalizing the Good Faith Estimate Workflow
At this stage, most practices either gain control or lose it. The rules for charging self-pay patients only work if your estimate process is built into daily operations. If the GFE lives outside the practice management system, depends on manual emails, or starts after clinical review is complete, your staff will miss it.
Operationally, the workflow should be built around upfront price determinism. If a service is scheduled less than 3 business days in advance, a GFE is not required, but for scheduled care the estimate must be prepared before service and the provider must maintain documentation needed to justify any variance from the estimate, according to this operational summary of the GFE timing and documentation rules.
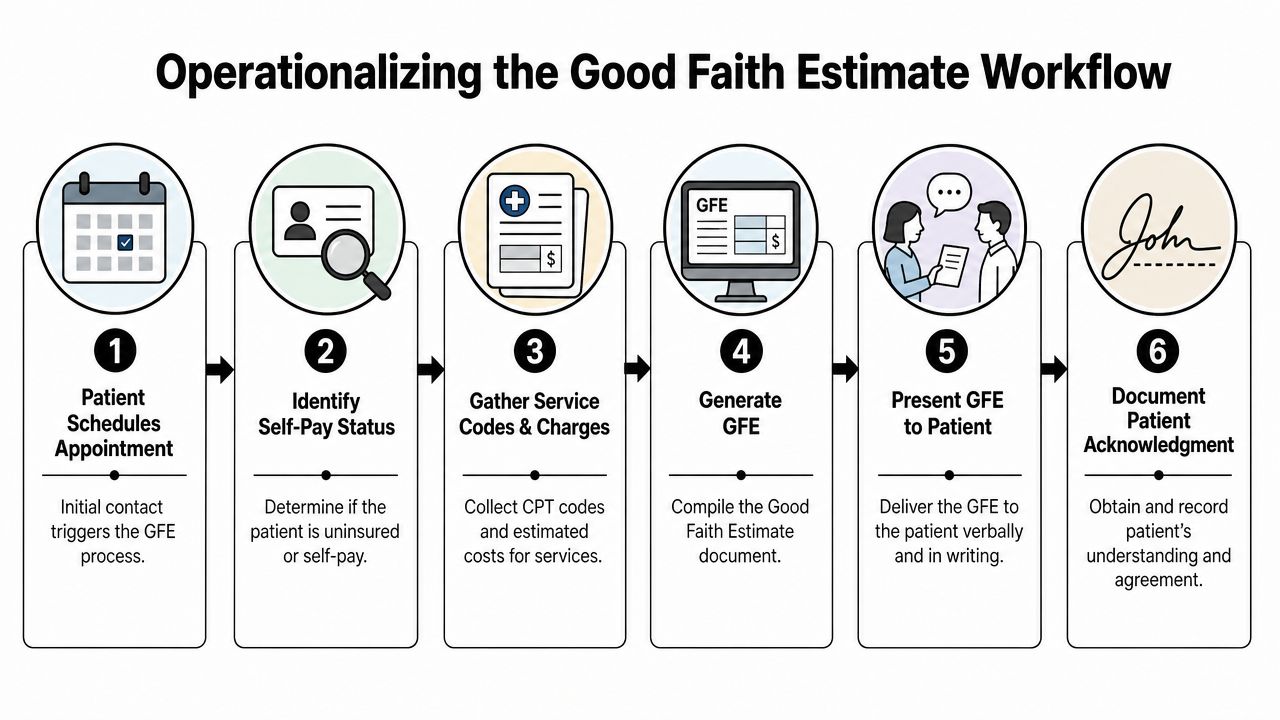
Step one starts at scheduling
The front end has to identify self-pay status immediately. Don't leave that decision for registration or billing.
Your scheduler should answer a few operational questions before the appointment is finalized:
- Is the patient uninsured or choosing not to bill insurance
- Is the service scheduled far enough in advance for the GFE requirement to apply
- Is the visit a simple office encounter or a multi-component procedural case
- Will other departments or rendering professionals contribute charges
If your PM system or EMR can't flag self-pay accounts at the time of booking, fix that before you do anything else. A compliant estimate process can't ride on free-text notes.
Build a controlled estimate engine
The GFE should come from standardized templates and approved charge logic, not from scratch. Specialty groups should maintain estimate templates by visit type, procedure family, and bundled service pattern. That's the only way to keep output consistent.
Here's the sequence I recommend:
- Flag the account early in the scheduling workflow.
- Pull expected services using likely CPTs, standard ancillary items, and known provider components.
- Apply the approved self-pay fee schedule rather than gross billed charges.
- Generate the written GFE using a standard template with itemized expected charges.
- Deliver and log it in a way you can prove later.
- Route exceptions to a financial counselor or designated billing lead.
Don't skip proof of delivery
A GFE that your team “probably sent” won't help you.
You need a record showing when the estimate was issued, how it was delivered, what version was sent, and whether the patient acknowledged receipt. That proof should sit in one place your billing team can access when questions arise. If your current systems scatter this across email, scanned PDFs, and phone notes, you're creating avoidable failure points.
The strongest estimate process is the one your billers can reconstruct in minutes without asking five people what happened.
Prepare for variance before service happens
The smartest practices don't wait until the claim drops to explain why the bill changed. They define variance triggers ahead of time.
Examples include a clinically necessary add-on service, a procedure that became more extensive than expected, or an ancillary item that wasn't reasonably known at scheduling. The point isn't to predict every scenario. The point is to decide in advance how your team will document the reason, who reviews it, and how the patient is informed.
A clean workflow has these characteristics:
| Workflow element | Required behavior |
|---|---|
| Self-pay identification | Automatic at scheduling |
| Estimate source | Approved fee schedule and templates |
| Timing control | Triggered before service when applicable |
| Delivery record | Time-stamped and retained |
| Variance management | Standard documentation path |
| Staff accountability | Named owners at each handoff |
If your estimate workflow still depends on memory, it will fail under pressure. Build it into the system and make it the default path.
Best Practices for Post-Service Billing and Collections
A clean estimate doesn't guarantee a clean payment. The handoff from pre-service financial counseling to post-service billing is where many practices undo their own good work.
Patients don't object only to high balances. They object to balances that feel unexplained. If the final statement looks disconnected from the estimate, collections slow down, calls increase, and staff start making side deals to get the account resolved.
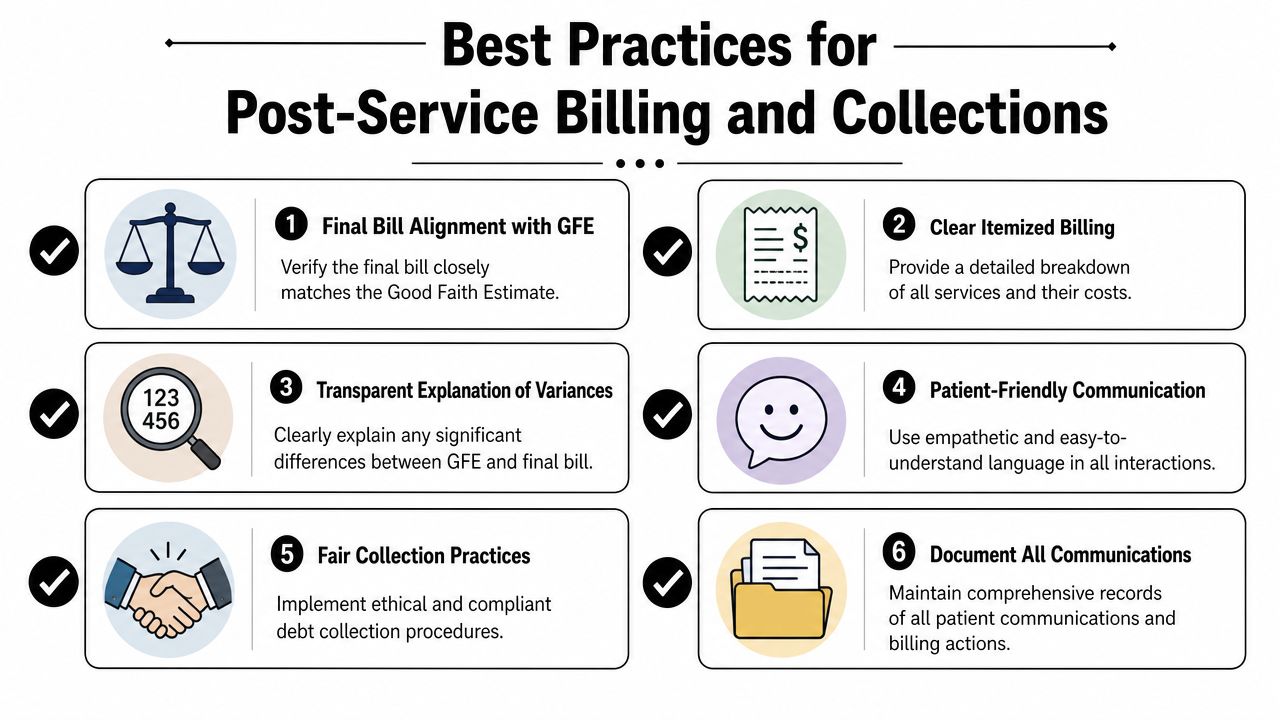
Keep the final bill recognizable
Your post-service statement should look like the natural continuation of the estimate, not a separate financial universe.
That means the final bill should use clear itemization, familiar service descriptions, and a visible link to what was discussed before care. If there's a difference, explain it plainly. Don't make the patient decode modifier logic or internal coding changes. Your staff may understand why the charge moved. The patient won't.
Use collections tactics that preserve the account
Aggressive collection behavior is often a sign that the front-end process failed. If the patient never understood the amount, a hard collection push usually hardens resistance.
A better approach is structured and transparent:
- Send the statement quickly while the visit and estimate are still fresh.
- Include itemized detail instead of broad category labels.
- Flag any variance early with a short explanation from billing, not after multiple patient calls.
- Offer payment arrangements consistently under a written policy.
- Keep every conversation documented so your team isn't restarting the explanation each time.
If your team handles a meaningful volume of patient balances, this overview of specialized patient collections support is worth reviewing to compare your internal process against a more disciplined revenue-protection model.
Financial assistance should be real, visible, and consistent
Many practices mention financial help only after an account is already delinquent. That's backwards.
If your organization offers financial assistance, hardship review, or structured payment plans, those options should be visible before collections get adversarial. The policy doesn't have to be complicated. It has to be accessible, documented, and applied consistently.
Here's the practical standard:
| Post-service area | Strong practice |
|---|---|
| Statement design | Itemized and easy to compare with estimate |
| Variance communication | Proactive explanation before dispute escalates |
| Payment options | Written plan rules, not verbal improvisation |
| Assistance policy | Available and communicated early |
| Account notes | Complete log of calls, letters, and payment discussions |
A patient is far more likely to pay a bill they understand than a bill your staff has to defend three different ways.
The revenue lesson
Collections performance on self-pay accounts is set earlier than most leaders think. If the estimate was accurate, the bill is clear, and the payment policy is consistent, your collections team can act like problem-solvers. If those pieces are weak, they become damage control.
That's why post-service billing isn't separate from compliance. It's where your process proves whether it was built correctly in the first place.
Building an Audit-Ready Documentation Trail
A patient disputes a self-pay balance six months after treatment. Your billing manager remembers the case. Your registrar remembers the conversation. None of that protects you if the file is incomplete.
Self-pay compliance lives or dies in the record. The file has to show the legal requirement, the workflow step, and the revenue decision in one clear timeline. If those pieces sit in different systems with no reliable trail, you create collection risk, refund risk, and audit exposure.
What belongs in the file
A defensible self-pay file should let an external auditor read the account from start to finish without calling your staff for context.
At minimum, include:
- The final Good Faith Estimate sent to the patient
- Proof of delivery showing when and how it was issued
- Any patient acknowledgment or signed financial agreement
- The final itemized bill
- Account notes for all billing-related communications
- Clinical or operational support for any material variance
- Approval records for discounts, payment plans, or hardship adjustments
Then make the file easy to retrieve. Set one storage standard, one naming convention, and one owner for completeness review. If the estimate sits in the PM system, the signed agreement is scanned into the EHR, and the variance explanation lives in email, your process is not defensible. It is fragmented.
Build files for disputes and audits
Documentation has one job. It must prove that your team followed policy and billed according to a documented method.
That means your record should answer basic questions fast. What did the practice know before service? What amount did the patient receive in writing? What changed? Who approved the change? When was the patient notified? Why does the final balance match your fee schedule, discount policy, and account notes?
Every self-pay file should be assembled as if it will be read by an external auditor with no prior context. If the account only makes sense after a verbal explanation from your billing office, the workflow failed upstream.
Standardize retention and test retrieval
Retention rules matter, but retrieval discipline matters just as much. A complete file that takes three days to assemble still weakens your position in a dispute.
Run periodic internal audits on recent self-pay encounters. Pull the record without warning. Confirm that staff can produce the estimate, delivery evidence, financial consent, itemized bill, variance support, and adjustment approvals from the same workflow path. If anything is missing, fix the process step that caused the gap. Do not just patch the chart.
For practices tightening controls across registration, estimating, billing, and collections, this framework for medical billing compliance operations is a useful benchmark.
Fast retrieval, clear chronology, and complete support turn documentation into revenue protection. Missing pieces turn every disputed balance into a negotiation.
Frequently Asked Questions About Self-Pay Rules
Gray areas come up fast in specialty care. The answer usually isn't to improvise. It's to apply the same principles consistently.
How should we handle recurring services or long treatment plans
Use a structured estimate process tied to the expected course of care. Don't rely on a single casual quote for a treatment series.
If the services repeat in a predictable pattern, build a documented estimate approach around that pattern and make sure the patient understands what is included, what may vary, and how changes will be communicated. Consistency matters more than clever wording.
What if an unexpected but necessary service is identified during the procedure
Document the clinical reason immediately and route the account for variance review. The billing office shouldn't be left to guess why the final amount changed.
Your file should show that the additional service was medically or operationally necessary, not included solely because it was billable. Then your post-service communication needs to explain that difference in plain language before the patient discovers it on a statement.
What if a patient says they're self-pay and later turns out to have insurance
Freeze the account and verify facts before posting forward with a self-pay collection path. In such situations, weak registration discipline creates downstream rework.
Your policy should define who updates the account class, whether prior estimates need revision, and how any payments already collected are handled. Don't let the team treat this as a clerical correction. It affects billing path, patient communication, and account integrity.
Do we really need coding discipline for self-pay accounts
Yes. Absolutely.
Self-pay doesn't mean unstructured. You still need accurate coding, consistent charge capture, and clean documentation of what was expected and what was performed. Otherwise, your estimate quality drops, your final bill becomes harder to defend, and your reporting loses value.
What's the simplest way to reduce self-pay disputes
Tighten three things first:
- Use an approved fee schedule
- Generate written estimates from standard templates
- Require proof of delivery and variance documentation
Most self-pay disputes come from process drift. Fix the workflow and the account follows.
RevGuard helps provider groups build revenue-protective workflows that hold up under scrutiny, from front-end RCM controls through dispute-ready billing operations and No Surprises Act enforcement. If your self-pay process still depends on manual estimates, scattered documentation, or reactive collections, RevGuard is worth a serious look.