
An air ambulance claim used to have a familiar arc. The transport happened under urgent conditions. The payer processed the claim out of network. The reimbursement came in low or late. Then the provider had one ugly fallback that often kept cash moving: bill the patient for the balance and fight the complaint later.
That workflow is gone for covered air ambulance claims. If you're responsible for ambulance revenue, the No Surprises Act didn't just add a legal rule. It rewired who carries the payment risk, how reimbursement disputes get resolved, and where your revenue cycle can fail.
Most public guidance on the No Surprises Act ambulance issue stops at patient protections. That's useful, but it doesn't answer the operational question providers face: how do you protect reimbursement when the patient is no longer the pressure point, the payer is, and the dispute process is highly structured?
The End of Surprise Ambulance Bills Or Is It
Before federal reform, ambulance billing generated constant friction. Patients often received bills they never expected, and providers often relied on post-service patient collections as part of the financial recovery model. A Harvard analysis noted that nearly 80% of ambulance rides resulted in out-of-network bills, with an average surprise bill of about $450 in its discussion of the situation before reform and later federal response to surprise billing in emergency care and air ambulance services, while also noting the continued ground ambulance gap in federal law (Harvard Petrie-Flom analysis).
For providers, that older model was messy but straightforward. If the payer underpaid, denied, or delayed, the account often shifted toward patient balance billing or extended collection activity. It created reputational risk, regulatory pressure, and ugly patient experience problems, but it was still part of the revenue toolkit.
Then the No Surprises Act took effect on January 1, 2022. For covered air ambulance services, the patient protection piece is clear. The revenue consequence is less widely understood. The law removed a major recovery lever and pushed the payment conflict into a payer-provider dispute framework.
What changed in practical terms
The central shift is this:
- Patients became more insulated: for covered air ambulance services, the patient isn't the balance-billing backstop.
- Payers became the primary battleground: if reimbursement is inadequate, the fight moves to plan adjudication, negotiation, and formal dispute channels.
- RCM quality became more important: weak documentation, coding errors, and avoidable denials hurt more when patient recovery is off the table.
Covered air ambulance claims didn't become simple after the NSA. They became more technical.
That matters because many organizations still run ambulance claims with a legacy mindset. They treat NSA compliance as a disclosure issue or a legal checkbox. It isn't. It's a reimbursement architecture issue.
What works and what doesn't
A provider survives this environment by tightening front-end intake, submitting clean claims, validating how the payer priced the service, and escalating underpayments quickly when the file supports it. What doesn't work is the old reactive pattern: send the claim, wait, complain about a low payment, then scramble for documentation after the dispute has already started.
For air ambulance providers, post-NSA success depends less on collection pressure and more on disciplined revenue engineering.
The Great Divide Air vs Ground Ambulance Rules
The most common mistake in any no surprises act ambulance discussion is treating air and ground transport as if federal law handles them the same way. It doesn't.
Consumer-facing coverage often says "ambulance" broadly, which causes confusion inside provider operations too. A major gap in public understanding is that ground ambulance bills are not covered by the federal law, and many people assume the law protects ambulance services broadly when in practice it mainly protects air ambulance claims (HealthInsurance.org glossary on the No Surprises Act).
Air ambulance under federal law
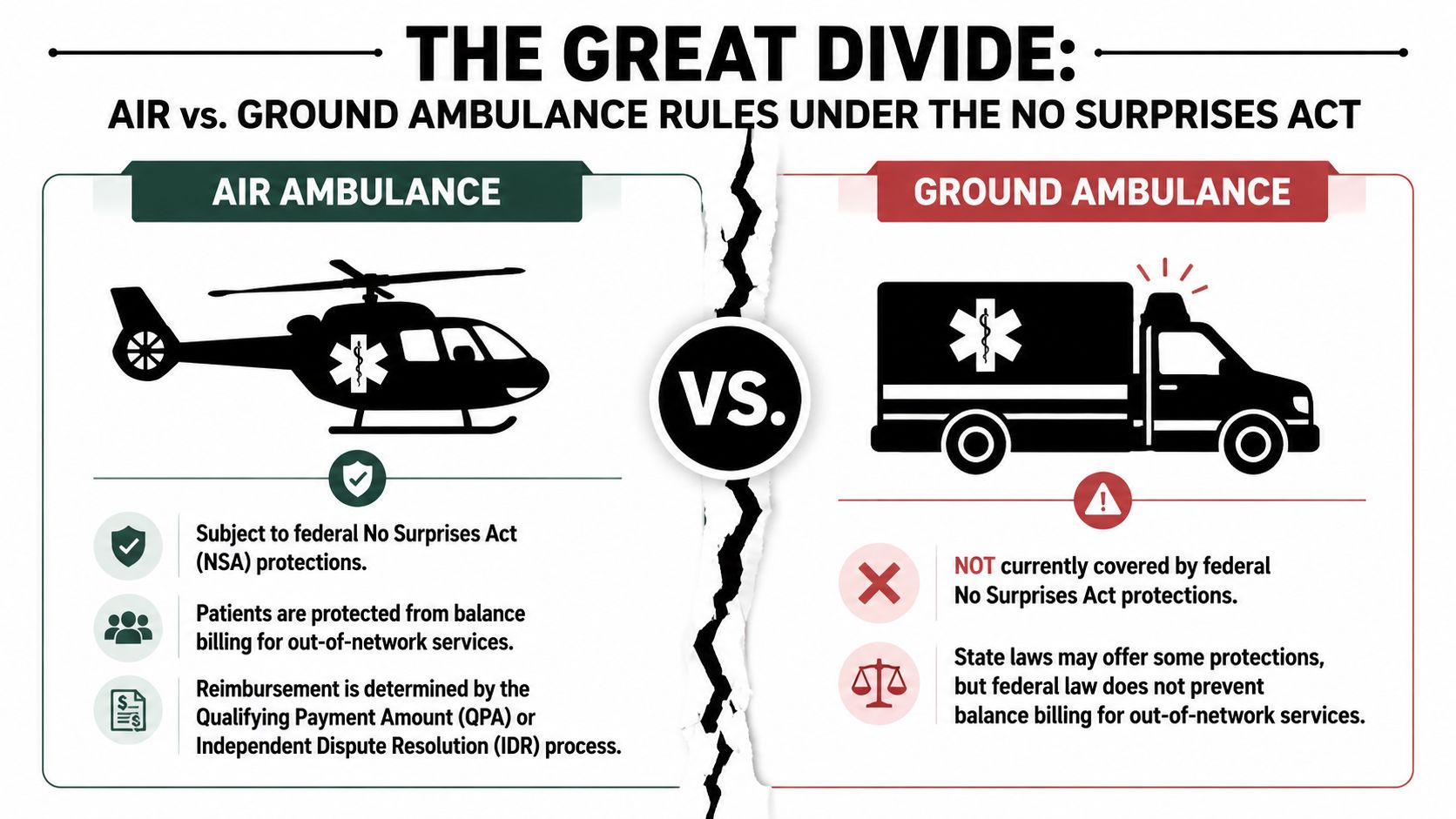
For out-of-network air ambulance services, the federal rule changes the claim path substantially. The provider can't rely on balance billing for covered services. The claim has to move through insurer adjudication and, if needed, formal payment dispute channels.
CMS training materials make the operational carve-out explicit: out-of-network air ambulance providers are barred from balance billing the patient, and those reimbursement disputes are resolved between the provider and the plan or issuer. Providers must bill the plan directly to trigger the law's payment mechanics, which shifts the workflow toward claim submission, adjudication management, and dispute documentation rather than downstream patient recovery (CMS NSA training material).
Ground ambulance outside the federal framework
Ground ambulance is different. Federal balance-billing protections under the NSA don't apply. That leaves providers and patients in a fragmented system shaped by state law, local regulation, payer behavior, and contract structure.
A useful way to think about it is this:
| Service type | Federal NSA balance-billing protection | Main payment pressure point |
|---|---|---|
| Air ambulance | Yes, for covered out-of-network claims | Payer adjudication and dispute resolution |
| Ground ambulance | No federal protection | State rules, contract terms, and patient billing exposure |
That divide creates two separate compliance and reimbursement playbooks inside one organization.
Why this divide matters to RCM
If your billing team treats all ambulance claims the same, you'll create avoidable errors.
- Air claims need NSA-specific workflows: claim review, patient statement controls, payer notice review, and dispute readiness.
- Ground claims need jurisdiction review: state consumer protection rules, plan type analysis, and local billing limits can matter more than federal NSA logic.
- Training has to split by service line: one script for air and another for ground is often necessary for both billing staff and patient-facing teams.
When teams blur air and ground rules, they usually create one of two problems. They either under-collect on ground claims or overstep on air claims.
The legal distinction is clear. The operational risk comes from acting as if it isn't.
Understanding Air Ambulance Patient Protections
For covered services, the patient-facing rule is the easy part to state and the easy part to violate if your billing system isn't configured correctly.
The No Surprises Act took effect on January 1, 2022 and protects people from surprise medical bills for out-of-network air ambulance services. For covered services, patient cost-sharing is limited to what they would pay for an in-network provider, according to CMS's explanation of patient rights under the NSA.
What the billing office must do
If you're billing a covered air ambulance claim, the patient should not receive a balance bill for the out-of-network difference. That means your patient accounting system can't default to the old logic of charging billed charges less payer payment.
Instead, the patient responsibility must reflect the applicable in-network cost-sharing amount under the plan. Operationally, that affects statement generation, collection workflows, call-center scripting, and refund handling if the wrong balance was billed.
For teams that need a more detailed operational discussion focused specifically on air transport, this air ambulance NSA compliance overview is a useful companion resource.
Where providers still get tripped up
The most common failures aren't legal theory problems. They're system and workflow failures:
- Legacy statement logic: patient balances generate automatically based on charge minus payment.
- Poor plan identification: staff don't flag that the claim falls within the air ambulance NSA framework.
- Collections misfires: a patient receives follow-up notices on a balance that shouldn't have been pursued.
- Misaligned call-center scripts: staff explain the account as an ordinary out-of-network bill.
Practical rule: If the patient statement is driving your reimbursement strategy on a covered air ambulance claim, the process is already off track.
What this means financially
The patient-protection rule changes your cash expectations. Patient collections are narrower on covered claims, so the payer-side reimbursement path carries more weight. That increases the importance of clean claim submission and disciplined follow-up.
Many organizations misread the law in this critical area. They focus on what they can't bill. The smarter move is to redesign around what they now must prove.
The New Reimbursement Benchmark The QPA
Once patient balance billing is restricted for covered air ambulance claims, the next question becomes straightforward: what anchors the payment dispute?
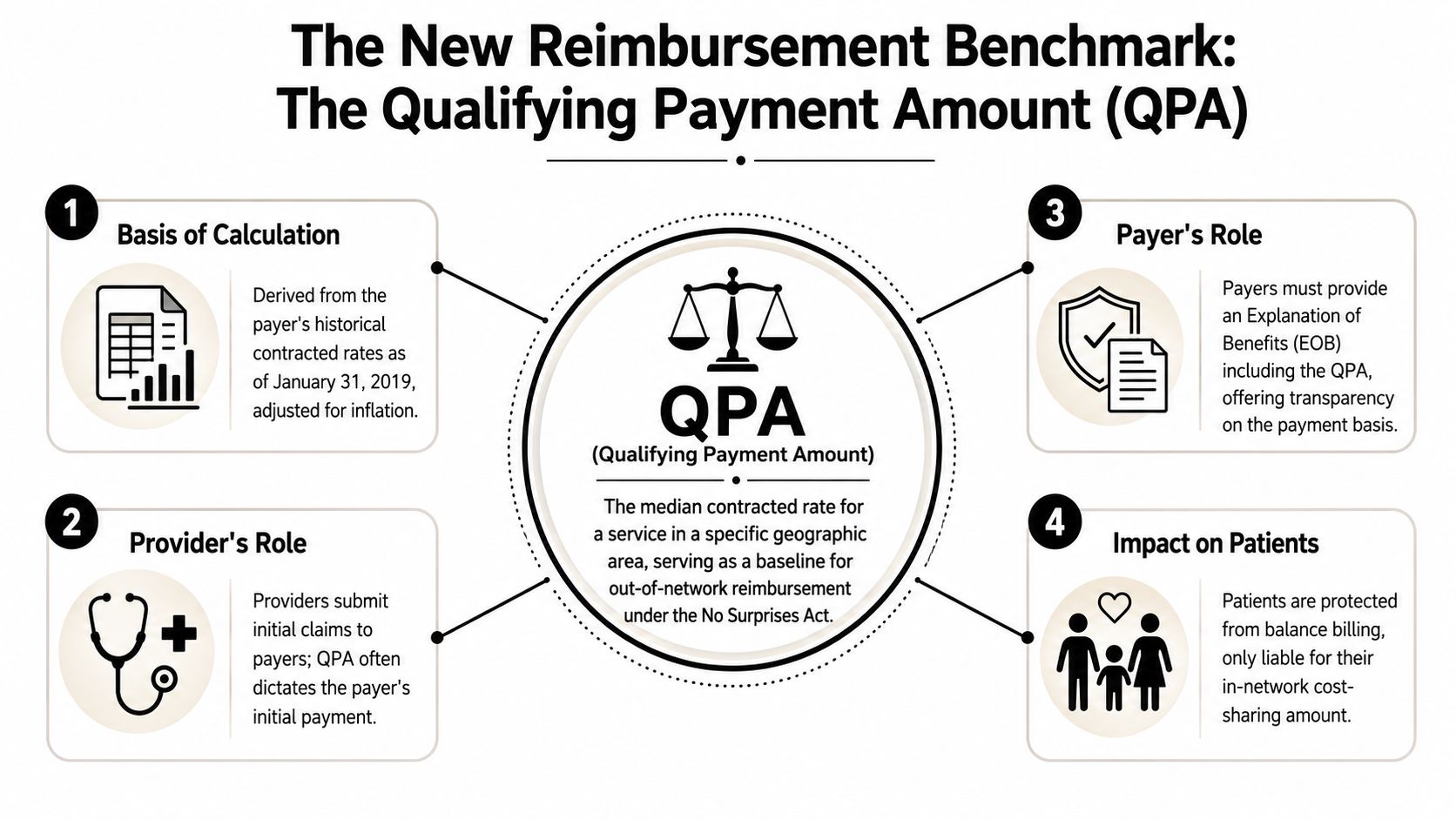
For covered No Surprises Act claims, the benchmark is the Qualifying Payment Amount, or QPA. The Department of Labor describes it as generally the plan's median in-network contracted rate for the same or similar service in the same geographic area, and the federal dispute process compares the parties' offers against that benchmark (Department of Labor overview of surprise healthcare expenses).
Why the QPA matters operationally
The QPA isn't just a legal concept. It affects how you evaluate the first payment and whether a dispute is worth pursuing.
If the payer's initial payment appears low, your team shouldn't jump straight to outrage. Start with a disciplined review:
- Confirm claim integrity. Was the code set complete, accurate, and supported by the record?
- Review the payer's notice. Did the plan identify the benchmark information needed to understand how it priced the claim?
- Compare service circumstances. Geographic area, service type, and coding details all matter when evaluating whether the payment aligns with the benchmark framework.
A lot of providers still analyze these claims against billed charges alone. That's usually the wrong lens in the NSA environment. The QPA-centric structure means the argument has to be built around claim facts, market context, and why the payer's position doesn't reflect the service appropriately under the statutory framework.
What providers should document early
A weak file at the start becomes a weak dispute later. Build the record before the underpayment battle begins.
- Service coding support: keep coding rationale and documentation aligned.
- Transport specifics: preserve dispatch details, timing, mission documentation, and clinical support records.
- Geographic context: maintain records that help establish where the service belongs for reimbursement comparison purposes.
- Contract intelligence: if your organization has relevant payer contract context, keep it accessible for escalation.
The QPA doesn't make reimbursement predictable. It makes the dispute more structured.
Common mistake
The biggest mistake is treating the QPA as untouchable. It is important, but it isn't the end of the analysis. A provider's task is to understand how the payer used it, whether the underlying categorization fits the claim, and whether the supporting record justifies a more favorable payment position.
That takes billing discipline, legal awareness, and evidence that can survive scrutiny.
Navigating the Independent Dispute Resolution Process
The NSA changed the pressure point for covered air ambulance claims, but it didn't guarantee payment. One industry explainer states directly that the law protects patients from out-of-network charges but does not guarantee that the insurer will pay the claim, set the reimbursement amount, or prevent claim denials, and federal guidance confirms that air ambulance providers can't bill patients for covered services yet may still dispute what the plan pays (AirMedCare Network explanation of air ambulance costs under the NSA).
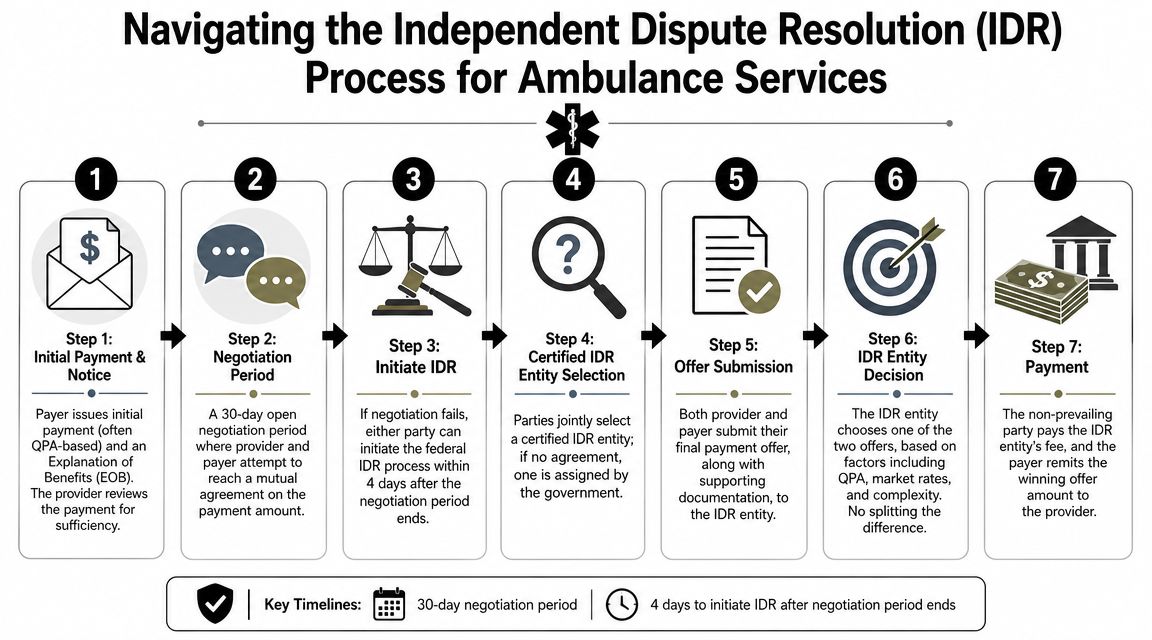
That's why the Independent Dispute Resolution, or IDR, process matters so much. For many air ambulance providers, it isn't a niche legal option. It's the formal payment correction mechanism when negotiation fails.
How the process functions in practice
An air ambulance claim is submitted. The payer issues an initial payment or denial with its explanation. If the provider believes the amount is inadequate, the parties move into a negotiation path before formal arbitration.
The strategic reality is simple. IDR rewards preparation, not indignation.
What strong providers do before filing
A good IDR submission usually starts long before anyone opens the portal. The strongest organizations build a dispute file while the claim is still in ordinary follow-up.
That means assembling:
- Clean clinical support: enough detail to support the coded service and the urgency of the transport.
- Adjudication history: notices, payment rationale, denial rationale, and any payer correspondence.
- Negotiation record: documentation showing the provider engaged the payer position before escalation.
- Payment theory: a concise explanation of why the provider's offer is more appropriate than the plan's.
Some organizations lose winnable disputes because their submission reads like a complaint letter. Others lose because the file is technically complete but commercially incoherent. The best filings are organized, fact-driven, and tied closely to the benchmark framework discussed earlier.
Where disputes break down
The recurring weak points are familiar:
| Failure point | Why it hurts |
|---|---|
| Missing documentation | The provider can't support the offer convincingly |
| Inconsistent coding narrative | The payer argues the service category or value is overstated |
| Late escalation | Internal delay weakens leverage and slows cash |
| Generic arguments | Boilerplate language doesn't distinguish the claim |
A low payment isn't the dispute. The documented explanation for why that payment is wrong is the dispute.
The teams that perform well in IDR usually have legal, coding, and reimbursement staff working from the same file. The teams that struggle often treat arbitration as a last-minute handoff.
Operationalizing Compliance An RCM Playbook
A claim enters the queue as an ambulance transport. If your intake team does not separate air from ground on day one, the account can move through the wrong edits, the wrong patient billing logic, and the wrong underpayment workflow before anyone catches it. By then, cash is delayed and correction costs more than the original process failure.
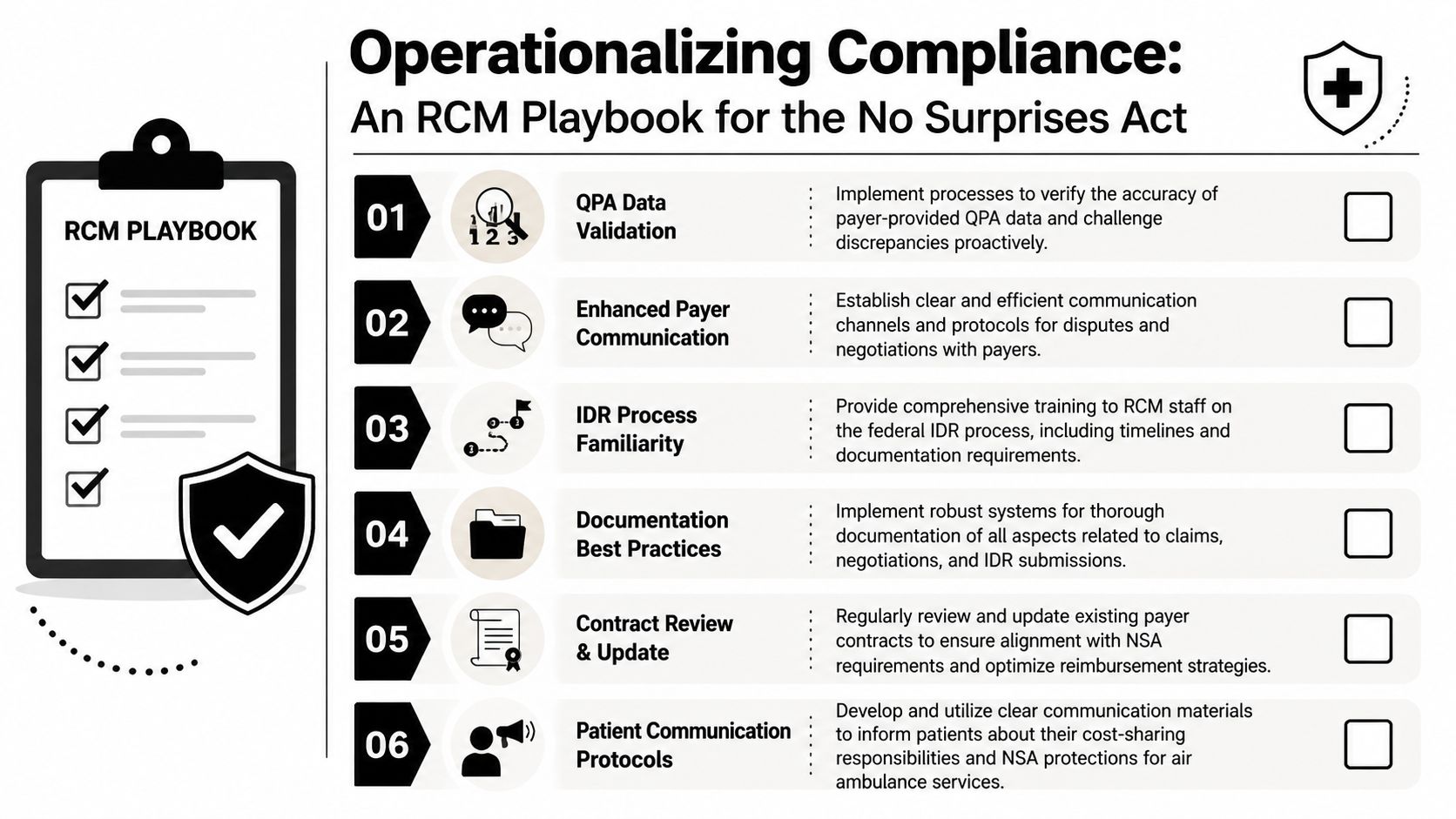
For covered air ambulance claims, compliance work and revenue cycle work sit in the same operating lane. The legal rule controls patient billing, payer response, staff scripting, file assembly, and escalation timing. Provider groups that treat those as separate handoffs usually create rework in every department.
Front-end controls
Start at intake, as preventable revenue loss usually begins there.
- Classify the transport correctly: split air and ground claims at the first touchpoint so each account follows the right billing and reimbursement rules.
- Verify plan details early: staff need enough coverage information to route the claim correctly and flag accounts that may trigger NSA-specific handling.
- Stop incorrect patient statements: covered air ambulance accounts should not flow into standard out-of-network balance billing logic.
These controls are simple. They also protect cash by keeping bad workflows from spreading downstream.
Mid-cycle claim discipline
Payers test file quality quickly, especially on higher-dollar transports. A technically submitted claim is not the same as a defensible claim.
Set a standard that every disputed air ambulance account must have a complete file in one place. That means coded claim detail, dispatch records, transport documentation, medical necessity support, EOBs, and payer correspondence are all retrievable without asking three departments to search their inboxes. If the documentation is scattered, underpayment review slows down and escalation deadlines get missed.
The operating rules should be plain:
- Coding must match the record. Internal inconsistency gives the plan an easy payment defense.
- Mission documents must stay together. Dispatch notes, logs, and clinical support should live in a single indexed file.
- Payer notices must be stored for retrieval. The dispute team should be able to pull every notice and payment rationale immediately.
- One owner must control underpayment review. Denials and underpayments often merge operationally. Someone needs authority to sort and escalate both.
Teams building that workflow can use this RCM readiness checklist for NSA IDR as a practical starting point.
Back-end underpayment strategy
Post-payment review needs a financial lens, not just a denial-management lens. The question is not only whether the claim paid. The question is whether the payment outcome matches the billing rule, the record, and the account's escalation path.
Use a triage model that separates fixable defects from true payment disputes:
- Administrative errors first: registration mistakes, missing data, and claim edits should be corrected fast so avoidable aging does not build up.
- Coverage and medical necessity issues next: these require documentation review and a payer-specific response.
- NSA-related payment disputes after that: escalate only when the file is complete enough to support negotiation or formal dispute activity.
This ordering matters. If staff send weak files into escalation, the provider loses time, weakens its position, and turns recoverable claims into write-off candidates.
Contracting and communication
NSA rules did not make payer contracts less important. Contracts still shape related reimbursement terms, operational obligations, and account handling decisions inside the billing office. I usually tell provider groups to review contract language and NSA workflows together, because staff errors often start where those two sets of rules conflict.
Patient communication needs the same discipline. For covered air ambulance claims, statement language, call-center scripts, and financial counseling should explain cost-sharing clearly and avoid suggesting that ordinary out-of-network balance billing applies. A bad script creates compliance risk. It also creates avoidable complaints and slows collections on amounts the patient does owe.
RevGuard is one example of a vendor model that combines ambulance-focused RCM workflow support with NSA and IDR operations. For some provider groups, that structure fits better than splitting claim operations, compliance review, and dispute preparation across separate vendors.
Securing Your Revenue in the Post-NSA World
The post-NSA environment isn't a softer reimbursement environment for ambulance providers. It's a more disciplined one.
For covered air ambulance claims, revenue risk shifted away from patient balance billing and toward payer behavior. That means the organizations that perform well aren't necessarily the ones with the loudest appeals. They're the ones with the best claim construction, the cleanest documentation trail, and the fastest escalation path when reimbursement doesn't match the service.
Ground transport remains a separate strategic issue. State and policy follow-through has been uneven. Commonwealth Fund reported that 18 states had some form of ground ambulance protections for fully insured plans as of its 2023 update, and it also noted that the federal Ground Ambulance and Patient Billing advisory committee approved recommendations in fall 2023 on protecting consumers from ground ambulance surprise billing (Commonwealth Fund update on ground ambulance protections). That doesn't create a uniform national payment standard, so providers still need a state-aware strategy for ground claims.
The durable operating model
The practical model is straightforward:
- classify ambulance claims correctly at intake
- control patient billing for covered air claims
- review payer pricing with QPA awareness
- build every contested claim as if it may need formal dispute resolution
- connect denial management, underpayment review, and legal escalation into one process
If those functions sit in separate silos, cash slows down and avoidable write-offs creep in. A tighter approach to healthcare denial management usually improves NSA performance because the same habits that reduce denials also strengthen underpayment disputes.
The NSA didn't eliminate ambulance payment conflict. It relocated it and formalized it.
Provider groups that understand that shift can still protect reimbursement. The ones that don't usually discover the problem after the patient balance is gone, the payer has anchored low, and the file isn't strong enough to push back.
If your organization needs a more durable way to manage air ambulance reimbursement under the No Surprises Act, RevGuard offers a model that links front-end RCM, underpayment detection, and NSA dispute execution in one workflow. That kind of integration helps providers reduce preventable leakage before a claim turns into an arbitration file, and it gives finance, billing, and compliance teams a clearer path when payer reimbursement falls short.