
You're probably living some version of this already. Patients are seen, notes are half-finished, your front desk is answering phones, and someone is staring at an explanation of benefits that looks like it was written to waste your afternoon. Claims go out late. Denials come back with vague reasons. Patient balances sit untouched because nobody wants the argument at checkout.
That isn't a paperwork problem. It's a revenue problem.
I've seen chiropractic clinics blame “insurance” for weak cash flow when the underlying issue was a fragile billing process. The leak usually starts upstream. Eligibility wasn't verified correctly. Visit limits weren't checked before treatment. Documentation didn't clearly support active care. A claim got submitted anyway, then denied, then appealed badly, then written off without fanfare. The practice owner never sees the full chain. They just feel the squeeze in payroll week after week.
That's why chiropractic billing services matter. Not because they take busywork off your plate, though they do. They matter because chiropractic reimbursement is rule-bound, denial-prone, and unforgiving when your documentation and billing workflow drift out of sync. If your billing operation can't produce clean, defensible claims and recover money when payers push back, you're financing your own underpayments.
Beyond Coding Crunches The True Cost of In-House Billing
The in-house billing story usually starts with good intentions. A chiropractor hires a reliable front desk lead, adds a billing module to the practice management system, and assumes the workflow will stabilize with enough repetition. For a while, it works. Then volume increases, payer rules shift, and the backlog starts creeping in.
The clinic owner notices symptoms before they identify the disease. Cash feels uneven. Staff stay late to fix claims. Patients get statements they don't understand. A denial sits untouched because nobody has time to call the payer. Another claim needs corrected modifiers, but the original note is vague. At that point, your billing team isn't managing revenue. They're triaging damage.
The hidden labor bill
Most clinics underestimate the cost of DIY billing because they only count wages. They don't count context switching, interruption, and rework.
A staff member who should be checking patients in is now chasing authorizations. A chiropractor who should be finishing exam findings is being pulled into coding questions. Your office manager is trying to reconcile payments, respond to patients, and figure out why the payer processed a visit as maintenance care. None of that shows up cleanly on a profit and loss statement, but you pay for it every day.
In-house billing rarely fails because your staff are lazy. It fails because chiropractic reimbursement punishes partial expertise.
Why chiropractic makes this worse
Chiropractic claims aren't simple data entry. The billing workflow has to connect clinical documentation to payer-specific coding, modifiers, and policy rules. If that connection is weak, the claim may be rejected even when the care itself was appropriate. That technical sensitivity is exactly why many clinics eventually look for specialized billing services for healthcare practices.
Here's the blunt truth. If your practice is submitting claims without tight control over eligibility, visit limits, authorization status, modifier use, and documentation support, you don't have a billing system. You have a delay machine.
What the financial leak looks like
The damage usually shows up in four places:
- Late filing pressure: Claims sit too long after the visit because notes aren't finished or nobody is available to scrub the claim.
- Preventable denials: The same categories keep recurring, but no one owns root-cause correction.
- Slow A/R cleanup: Old balances linger because follow-up happens only when someone “gets to it.”
- Patient collection friction: Patients lose trust when your office can't clearly explain what insurance covered and what it didn't.
A practice can survive with this setup for a while. It won't grow cleanly with it.
The Core Components of Chiropractic Billing Services
A real billing service isn't a claim-sending vendor. It's a financial pit crew. Every role exists to keep revenue moving, catch issues before they turn into denials, and clean up what slips through.
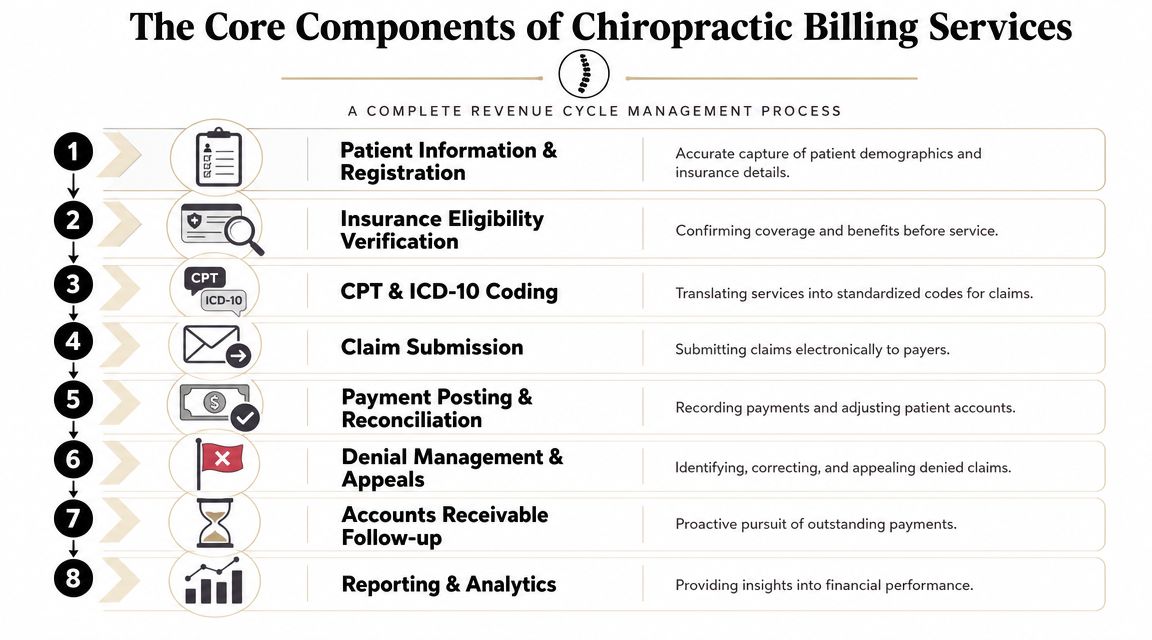
Front-end controls
The first job is patient and insurance intake. If demographics are wrong or the insurance card is entered carelessly, the claim starts broken.
Then comes eligibility verification. In chiropractic, this step matters more than many clinics admit. The billing workflow has to verify coverage, visit limits, and authorization rules before treatment because claims must map the clinical record into payer-specific ICD-10 diagnosis codes, CPT procedure codes, and modifiers. Errors in any of those fields can trigger denials, which is why strong workflows confirm those details before the visit and make sure the claim is supported by documentation and payer policy, as outlined in this overview of chiropractic billing requirements.
Mid-cycle execution
Once the patient is seen, coding and charge entry need to reflect what the record supports. Average billing teams often show their limitations at this point. They can key in codes. They can't always spot when the note fails to support the modifier logic or when the diagnosis linkage is weak.
A complete service typically handles:
- Coding review: Making sure diagnosis codes, procedure codes, and modifiers align with the note and payer expectations.
- Clean claim submission: Sending claims electronically with edits that catch obvious errors before the payer does.
- Payment posting: Reconciling payer payments and contractual adjustments against what was billed.
- Patient balance handling: Moving clean residual balances to the patient with understandable statements and consistent follow-up.
Back-end recovery
Good firms separate themselves from form submitters.
A serious billing partner works denied and underpaid claims with discipline. They identify why the claim failed, correct what can be corrected, and appeal when the documentation supports payment. They also monitor aging accounts so balances don't rot in receivables.
Practical rule: If a billing company talks mostly about claim submission and barely talks about denial recovery, they're selling production, not protection.
The strongest setups also report on payer behavior, denial patterns, and aging trends in a way your clinic can act on. That matters because billing shouldn't just tell you what happened last month. It should show you where revenue is getting stuck and who needs to fix it.
What you're actually buying
You're buying a sequence of controls, not a clerk. That distinction matters.
| Billing function | What it protects |
|---|---|
| Eligibility and benefit checks | Preventable front-end denials |
| Coding and modifier review | Claim accuracy and reimbursement support |
| Submission and edits | First-pass cleanliness |
| Payment posting and reconciliation | Revenue visibility |
| Denial management | Recoverable cash |
| A/R follow-up | Speed of collections |
| Patient statements | Downstream patient collections |
| Reporting | Accountability and process correction |
If your current “billing service” only handles two or three of those, it isn't full revenue cycle support.
Navigating Common Chiropractic Reimbursement Hurdles
Chiropractic claims don't get denied just because someone typed the wrong code. They get denied because the entire reimbursement chain is easy to break. The documentation may not show active treatment clearly enough. The payer may apply visit limits aggressively. Medicare may treat a service as non-covered while the practice bills it as if it were covered. Those are operational failures, not random bad luck.
Denials are common for a reason
Industry sources describe denials as a major operational problem. One source states that 5% to 10% of revenue claims are denied, and the same discussion says 30% of all chiropractic claims are denied on the first submission. That same revenue-cycle guidance recommends filing claims the same day the service is provided and keeping A/R days within 0 to 30 days to reduce cash-flow delays, according to ChiroTouch's discussion of chiropractic billing challenges.
That should reset how you think about billing. In chiropractic, denial management isn't a cleanup task. It's part of the core business model.
Active treatment versus maintenance care
This is one of the biggest fault lines in chiropractic reimbursement. The payer isn't just asking whether treatment occurred. They're asking whether the record proves medical necessity for active care.
If the documentation doesn't show measurable change, clear clinical rationale, and a treatment plan tied to functional improvement, the payer has a straightforward path to label the care maintenance. Once that happens, your appeal gets much harder. The note has to defend the claim, not merely describe the visit.
A billing service worth paying for will press your clinic on note quality, not just coding accuracy.
Medicare is where clinics get sloppy
A lot of practices know the shorthand. Use the AT modifier when appropriate. Link the diagnosis correctly. That's not enough.
CMS draws a sharp line between covered chiropractic manipulation and non-covered services. It also states that it is not appropriate to bill Medicare for services that are not covered as if they are covered, and it directs providers to use the proper non-covered billing pathways, as explained in the CMS Medicare coverage article on chiropractic services.
That means your team needs to know when patient liability should be handled through the correct non-covered route, including use of modifiers and notice workflows where appropriate, rather than pretending the service belongs on a standard covered claim.
If your Medicare workflow is “bill it and see what happens,” you have a compliance problem, not a billing strategy.
For practices dealing with repeated payer pushback, a structured healthcare denial management process matters because appeal discipline is often the difference between a write-off and a collectible balance.
Frequency limits and audit exposure
Another common trap is assuming that a paid claim is a safe claim. It isn't.
Payers review active-treatment compliance, visit frequency, and medical necessity over time. A clinic can submit a technically clean claim and still be vulnerable later if the documentation pattern looks like maintenance care or exceeds what the payer considers reasonable without strong support. That's why the best billing operations think beyond submission. They build records that can survive post-payment scrutiny.
Here's the practical standard I use when advising clinics:
- Check necessity early: Don't wait for denial language to tell you the note was weak.
- Watch visit accumulation: Frequency issues are predictable. Treat them like they're predictable.
- Separate covered from non-covered cleanly: Mixed workflows create both denials and patient confusion.
- Appeal from the chart, not emotion: Payers don't reimburse frustration. They reimburse supportable claims.
Pricing Models and Calculating Your Billing ROI
Chiropractic billing services usually use one of two pricing models. Neither is automatically better. The right one depends on your volume, your internal staffing, and how much variability you can tolerate in monthly billing costs.
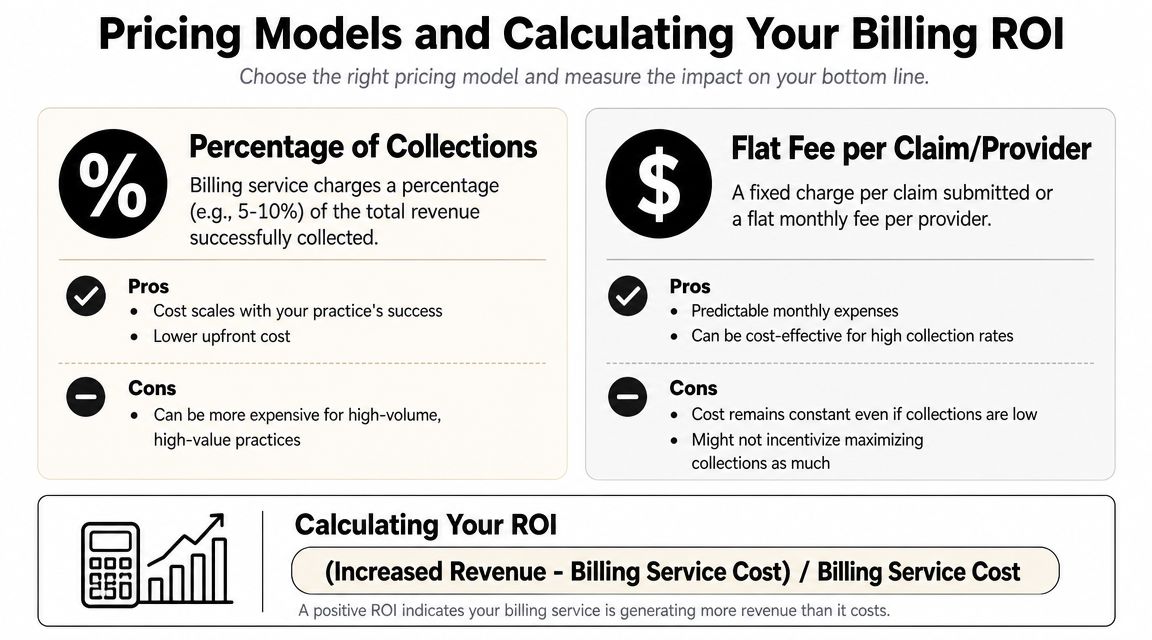
Percentage of collections versus flat fee
Reported market pricing commonly falls into two buckets. Some chiropractic billing companies charge a percentage of collections, with reported ranges of about 3% to 9% of collections. Others use a flat monthly fee, with pricing starting around $200 per month for solo practices and running $600+ for larger clinics. One cited example describes a 5-doctor clinic with 10,000 patients paying $1,200 per month for billing services, according to EMR Guides' review of chiropractic medical billing pricing.
Here's the plain-English comparison:
| Model | Good fit | Main upside | Main downside |
|---|---|---|---|
| Percentage of collections | Growing practices, uneven collections, owners who want aligned incentives | Cost rises and falls with cash coming in | High-volume clinics may pay more over time |
| Flat monthly fee | Stable practices with predictable volume | Easier budgeting | You pay the same even when collections dip |
My recommendation by practice type
I usually steer smaller or less stable clinics toward percentage-based pricing first. It protects cash flow during messy periods and aligns the vendor with collection performance.
I usually prefer flat pricing for disciplined clinics with strong front-desk processes, reliable documentation, and enough volume to make a fixed fee efficient. But only if the scope is clear. A cheap flat fee that excludes serious denial work is often expensive in disguise.
How to calculate ROI without fooling yourself
Most owners calculate billing ROI badly because they only compare vendor fees to payroll. That's too narrow.
Use this framework instead:
- Start with recovered revenue. Look at what your current process fails to collect but should.
- Add labor relief. Estimate staff time that moves from claim chasing to patient-facing work.
- Add error reduction value. Fewer corrected claims means fewer delays and fewer small write-offs.
- Subtract the billing service fee.
- Ignore fantasy gains. Don't assume dramatic improvement without proof.
Decision filter: If a billing company can't explain where your current leaks are, they can't build a credible ROI case.
A realistic way to compare proposals
When you review vendors, ask them to show how they handle these categories:
- Eligibility failure: Who checks benefits, visit limits, and auth status?
- Documentation mismatch: Who flags notes that won't support payment?
- Denial recovery: Who owns appeals, follow-up cadence, and payer escalation?
- Patient balances: Who manages statements and collections after insurance processing?
- Reporting: Do you get actionable dashboards or just a static summary?
The fee matters. The leak coverage matters more.
A slightly higher fee can still be the better deal if the company closes more revenue gaps, shortens collections lag, and keeps your team out of constant rework. A low monthly price looks attractive until you realize your staff are still doing half the job internally.
How to Evaluate and Select the Right Billing Partner
Monday morning. Your front desk is fielding patient calls, your CA is stuck on unpaid claims from last month, and your billing vendor just sent a tidy report that says claims were submitted on time. Meanwhile, cash is still slow, denials keep repeating, and no one can explain which cases are worth appealing and which notes were weak from the start.
That is the wrong standard.
A chiropractic billing partner should protect revenue under pressure. Submission speed matters, but recoverability matters more. If a company cannot defend medical necessity, respond to maintenance-care disputes, and work old A/R with discipline, it is not managing your revenue cycle. It is just moving claims through a pipe.
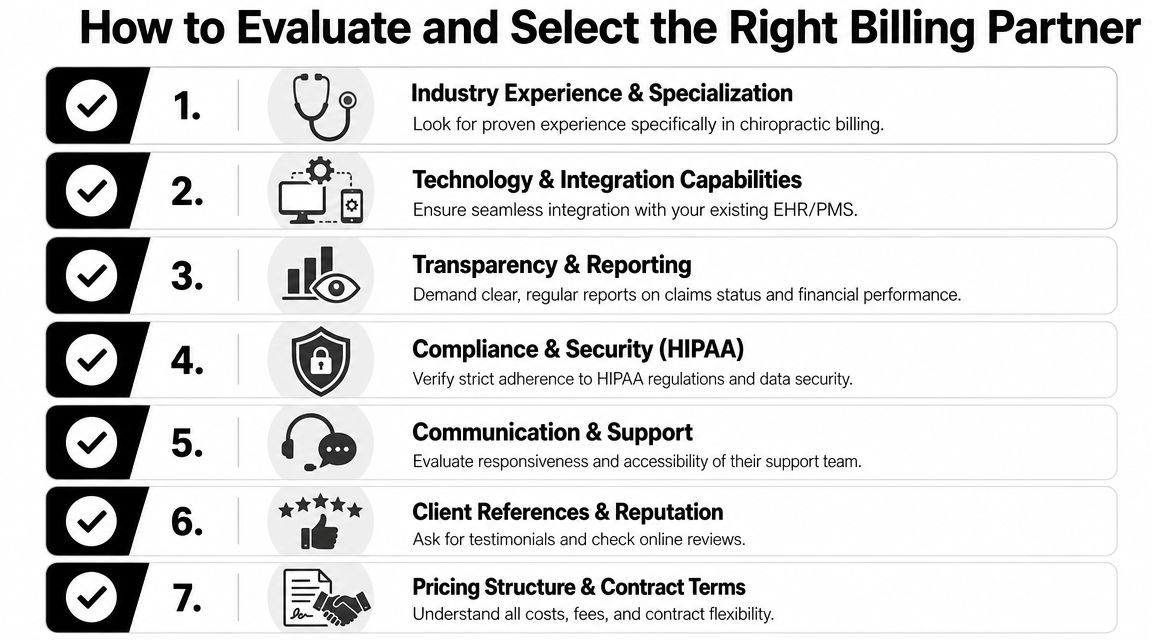
Start with specialty depth
Generic medical billing experience is not enough. Chiropractic reimbursement turns on details that many generalist vendors handle poorly. Your partner needs working knowledge of active treatment versus maintenance care, modifier use, payer-specific frequency rules, and the documentation patterns that trigger denials or post-payment reviews.
One industry source makes this point clearly. A major challenge in chiropractic billing is producing documentation that can hold up when payers question maintenance care or visit frequency, as discussed in MZ Billing's chiropractic billing overview. The better vendors build claims that are ready for scrutiny before they ever go out the door.
Use a checklist that tests operational control
A polished demo proves almost nothing. Use a checklist that shows whether the vendor can find leaks, prevent avoidable denials, and recover money after a payer pushes back.
- Specialty experience: Ask for chiropractic-specific examples, including denials tied to medical necessity, modifiers, and maintenance care.
- Documentation review process: Require a clear method for catching weak notes before claim submission.
- Appeal ownership: Ask who writes appeals, what records they pull, and how they decide whether a denial is worth fighting.
- A/R follow-up: Clarify who works aging balances, how often they follow up, and when they escalate.
- Patient balance workflow: Confirm how statements, calls, payment plans, and handoffs are handled after insurance processes the claim.
- Reporting visibility: Demand reporting that shows denial reasons, aging by payer, appeal outcomes, and unresolved claim categories.
- System compatibility: Ask whether they can work inside your current tools or whether they create friction by forcing a platform change.
- Collections support: If patient balances are a growing problem, ask how their workflow connects with medical collections software for healthcare practices.
- Compliance process: Verify how they handle HIPAA, access controls, and payer policy changes.
Ask questions that expose weak vendors fast
Broad questions get polished sales answers. Operational questions expose whether the team has a repeatable process or a script.
Use questions like these:
- Walk me through a medical-necessity denial from receipt to final resolution.
- How do you catch notes that read like maintenance care before the claim is filed?
- What is your process when a payer says visits exceeded frequency limits?
- Who owns old A/R, and what follow-up cadence do they use?
- How do you separate patient liability from covered billing in Medicare cases?
- What reports will I see every week or month, and what decisions should those reports drive?
A weak vendor talks about software and turnaround times. A strong one asks for denial trends, sample notes, payer mix, and your top write-off categories.
Buy process, not promises
Good billing companies can explain exactly how work moves from charge entry to denial recovery. They can show who owns each step, what triggers an appeal, when they escalate to the payer, and how they report progress back to the clinic.
This is also where you should compare operating models. Some firms stay focused on claim submission and standard follow-up. Others connect billing to payment dispute recovery and underpayment work. RevGuard, for example, offers billing services, clean claim submission, and dispute-oriented revenue workflows. This distinction is important for clinics wanting a partner that thinks past submission and toward recoverability.
Do not confuse a friendly sales process with a disciplined revenue process.
Red flags that should end the conversation
| Red flag | What it usually means |
|---|---|
| They brag about submission speed but say little about denials | They are built for throughput, not reimbursement defense |
| They do not ask for sample notes or denial categories | They are not diagnosing your specific revenue problems |
| Reporting stops at monthly summaries | You will not get enough visibility to fix issues quickly |
| They promise to “handle everything” without showing workflow ownership | Accountability will get blurry fast |
Choose the partner that treats billing like revenue protection. Chiropractic claims are challenged after submission, not just before it. Your vendor should be ready for that fight.
Integrating Billing Services with Your Practice Technology
Billing doesn't sit on top of your practice like a detachable accessory. It runs through your technology stack. If the data flow is sloppy, your billing partner spends their time cleaning up preventable errors instead of protecting revenue.
The three-system handshake
At minimum, chiropractic billing services need clean coordination across three environments:
- Your EHR or practice management system: Scheduling, demographics, notes, and charges begin here.
- The clearinghouse: This is the transmission layer that routes claims and returns payer responses.
- The billing team's workflow and analytics tools: Edits, follow-up, denial tracking, and reporting occur here.
If those systems don't talk cleanly, problems multiply fast. A diagnosis may not flow correctly from the chart. A modifier may be dropped or mismatched. A payer rejection may sit in a queue no one is actively watching.
Don't let the software dictate your business blindly
Some billing companies insist you use their preferred platform. That can work if your clinic is already planning a broader systems change and the new setup improves data quality.
But there's a trade-off. Forced migrations create training strain, temporary workflow confusion, and the risk of moving old problems into a new interface. In many cases, I'd rather see a billing partner integrate effectively with the clinic's current system than force a dramatic platform switch for the sake of vendor convenience.
Ask direct questions:
- What systems do you already support well?
- Where do claim edits happen?
- Who owns rejected-claim work queues?
- How do clinical notes reach the billing team for review when support is needed?
- How are payment postings and patient balances reconciled?
Dashboards matter more than pretty reports
A monthly PDF isn't enough. By the time it lands in your inbox, the operational damage is old news.
You want on-demand visibility into claim status, aging, denials, and payment trends. That's where a tool such as medical collections software for revenue visibility becomes relevant. The point isn't branding. The point is workflow transparency. If your billing partner can't show you where money is stuck right now, you're managing by hindsight.
A modern billing relationship should let you see your receivables as a living pipeline, not as last month's autopsy.
What smooth integration looks like
A well-integrated setup has a few clear traits:
| Integration area | Healthy sign |
|---|---|
| Patient demographics | Minimal duplicate entry |
| Clinical documentation | Billing team can verify support without chasing screenshots and emails |
| Claim status flow | Rejections and denials are visible quickly |
| Payment posting | Reconciliation happens consistently |
| Reporting | Dashboards are accessible and understandable |
Technology won't save a weak billing process. But weak technology handoffs will definitely sabotage a strong one.
Key KPIs to Monitor Your Billing Service Performance
If you outsource billing and then only glance at deposits, you're flying blind. Good revenue cycle oversight depends on a small group of metrics that tell you where claims are stalling, where denials are creeping in, and whether your partner is doing the work they promised.
Start with aging and denial visibility
The first KPI I look at is days in A/R. This measures how long it takes for billed charges to turn into collected cash. You already saw the operational standard earlier: disciplined chiropractic billing teams work to keep A/R moving quickly, not lingering in old buckets. If your aging keeps stretching out, ask why by payer, not just in aggregate.
The second KPI is denial rate by payer and reason. Don't accept a single blended number with no detail. You need to know which payers are denying, what categories are recurring, and whether the root cause is eligibility, coding, documentation, authorization, or follow-up failure.
Watch first-pass quality and net collections
First pass resolution rate tells you how many claims clear without needing correction or rework. A low result usually points to front-end intake gaps, coding mismatch, or weak note support.
Net collection rate or adjusted collection rate tells you how much of the collectible revenue you're bringing in after contractual adjustments. This metric matters because raw collections alone can hide preventable write-offs, weak follow-up, or sloppy patient balance handling.
Use KPIs to force useful conversations
Don't ask your billing partner whether things are “going well.” Ask these instead:
- Which denial categories increased this month, and why?
- Which payer has the oldest unresolved A/R?
- How many claims required correction after submission?
- What operational change inside my clinic would improve first-pass performance fastest?
That last question matters. Strong billing teams don't just report numbers. They translate numbers into clinic actions.
Owner mindset: A KPI is only useful if it leads to a process change, an accountability assignment, or a payer escalation.
Keep the dashboard simple
You don't need a wall of metrics. You need a working scorecard.
| KPI | Why it matters | What to ask |
|---|---|---|
| Days in A/R | Shows cash-flow speed | What's aging past expected follow-up windows? |
| Denial rate by payer and reason | Shows where claims break | Which categories are preventable? |
| First pass resolution rate | Shows claim cleanliness | What failed before submission? |
| Net or adjusted collection rate | Shows how much collectible revenue is actually captured | Where are we leaking collectible dollars? |
If your billing company can't speak comfortably about these metrics, they're not managing your revenue cycle with enough rigor.
Chiropractic Billing Services FAQ
What's the real difference between a billing service and a clearinghouse
A clearinghouse routes claims and returns payer responses. That's useful, but it's only one layer. A billing service handles the operational work around the claim, including claim review, denial follow-up, payment posting, A/R management, and patient balance processing. In short, the clearinghouse moves the file. The billing team manages whether the file gets paid.
How disruptive is it to switch billing services
It's disruptive if the transition is sloppy. It's manageable if the new partner has a clear handoff plan. The risk points are open claims, old A/R ownership, payer enrollments, data access, and staff confusion over who handles what. Before switching, require a written transition workflow, not verbal reassurance.
Will I lose control of my finances if I outsource
You'll lose control only if you outsource blindly. A good billing relationship increases visibility because you should get cleaner reporting, clearer accountability, and a more disciplined follow-up process. If a vendor becomes a black box, that's a bad vendor problem, not an outsourcing problem.
Should I choose a cheaper service if they say they can do the same work
Usually, no. In chiropractic billing, cheap often means narrow scope. If the low-cost vendor doesn't own denial recovery, documentation feedback, and aging follow-up, your staff will absorb the missing work internally. The invoice stays low while the revenue leak stays high.
If your clinic is tired of resubmitting the same problems month after month, it's worth talking to RevGuard. They work across billing, denial pressure, and revenue protection workflows, which is the right lens for practices that need more than claim submission.