
Claims adjudication cost providers more than $25.7 billion in 2023, and nearly $18 billion of that may have been unnecessary because many disputed claims were ultimately paid after review, according to a major hospital survey reported by Premier. That number should change how practice managers think about the claim adjudication process. This isn't a back-office event that starts after submission. It's a revenue event that begins at scheduling, registration, authorization, documentation, coding, and contract interpretation.
The mistake I see most often is treating adjudication as a payer-side black box and disputes as a separate downstream function. In practice, they're the same continuum. A claim that isn't built to survive edits, scrutiny, underpayment logic, and appeal review is already vulnerable before it leaves your system.
The organizations that recover more revenue usually don't “fight harder” only after the denial. They engineer dispute-readiness upstream. They capture the right eligibility detail, preserve authorization evidence, align coding to documentation, understand expected reimbursement logic, and create a paper trail strong enough to support reconsideration, appeal, or IDR if payment breaks the wrong way.
The High Cost of an Opaque Process
Seventy percent of denied claims were ultimately overturned and paid in a 2023 hospital survey reported earlier. That is a costly way to run revenue cycle operations.
The losses usually do not start with the remittance. They start in the gaps between teams and systems. A registration rep captures the wrong plan variant. Authorization proof stays in a payer portal instead of the patient account. Clinical documentation supports the service, but coding does not line up with how the payer applies edits. Payment then posts short, and the remit gives staff too little detail to tell underpayment from true noncoverage.
That sequence is what makes adjudication feel opaque. The payment decision appears at the end, but the preventable failure often sits upstream.
Why the cost burden matters
The financial issue is not just denial volume. It is avoidable rework on claims that were payable all along. Every corrected claim, reconsideration, appeal, and payer call adds labor cost, delays cash, and ties up staff who should be working cleaner accounts. For a practice manager, that shows up in higher A/R, less predictable collections, and more pressure on staffing.
I treat that as a design problem, not a collections problem. If a payer eventually pays after review, the original claim and account record were not built well enough to survive scrutiny on first pass. The operational fix is to make claims dispute-ready before submission, with clean eligibility data, preserved authorization support, documentation that supports code selection, and a clear expected reimbursement model.
Practical rule: If a denial is later overturned, your team spent money proving a claim that should have been easier to pay the first time.
Where opacity hurts margin
Opaque adjudication creates three forms of leakage:
- Administrative leakage when staff rework claims, retrieve missing records, and resubmit or appeal accounts that should have cleared on first submission.
- Timing leakage when delayed payment stretches A/R, distorts cash forecasting, and increases dependence on follow-up labor.
- Analytical leakage when vague remits and inconsistent payer reasoning prevent the team from identifying whether the actual issue is coverage, coding, contract application, or payment variance.
This gets more expensive in specialties and higher-acuity settings where reimbursement depends on fee schedules, carve-outs, modifiers, multiple procedure logic, or out-of-network methodology. If the team cannot define expected payment before the ERA arrives, underpayments blend in with routine posting. A working understanding of the insurance allowed amount gives staff a baseline for spotting variance early and building a supportable challenge when payment is wrong.
The shift that works
Strong teams treat adjudication, appeals, and IDR as one continuum. They do not wait for a denial to start assembling the file. They create a claim record that can stand up to payer edits, medical necessity review, underpayment analysis, reconsideration, and formal dispute review if needed.
That approach changes decisions upstream. Scheduling verifies the right coverage. Registration captures the data that will later support billing. Authorization evidence is stored where the billing team can retrieve it fast. Coding is checked against payer logic, not just code-set accuracy. Contracts and payment rules are translated into expected reimbursement so posting staff can identify variance on receipt.
That is how opacity loses its grip. The claim arrives at adjudication with the facts, support, and payment expectations already in place.
What Is Claim Adjudication and Its Objectives
The claim adjudication process is the payer's rules-based decision engine for determining financial responsibility on a submitted claim. The payer receives the claim, checks it against eligibility, benefits, coding logic, policy terms, and contract rules, then decides whether to pay, reduce, deny, or hold it for more information.
For providers, adjudication is the last gate before earned revenue becomes actual cash. For payers, it's the mechanism used to enforce coverage rules and payment policy.
A gatekeeper at massive scale
This isn't a niche administrative task. Policy research cited by One Percent Steps on real-time adjudication says U.S. insurers adjudicate over 3 billion medical claims each year, averaging about 10 claims per enrollee. The same research says administrative costs tied to adjudication can run $50 to $100 per claim, that about 80% of claims are adjudicated automatically, and roughly 20% require manual review.
That split matters operationally. A relatively small share of claims can consume a disproportionate amount of labor if they fail payer edits and move into exception handling.
The payer objective and the provider objective are not the same
A payer wants consistency against policy and payment rules. A provider wants timely, accurate reimbursement. Those goals overlap only partially.
Here's the practical difference:
| Perspective | Primary objective | Operational result |
|---|---|---|
| Payer | Apply benefit, coverage, and payment rules consistently | More edits, holds, reductions, and denials when required fields or logic fail |
| Provider | Convert documented care into collectible cash quickly | Stronger front-end controls, fewer edits, faster payment, less rework |
When practice managers miss that tension, they often assume a “clean billed” claim will be paid cleanly. That's not always true. A claim can be syntactically correct and still be vulnerable to payer logic around eligibility timing, authorization status, medical necessity interpretation, modifier use, or fee schedule application.
What adjudication is really deciding
The payer's system is effectively asking a short series of questions:
- Is this claim valid enough to enter processing?
- Was the patient eligible and was the service covered?
- Do the diagnosis, procedure, provider, and timing data fit policy rules?
- What amount, if any, is payable under the contract or plan terms?
- Does anything require a human reviewer to intervene?
A paid claim is not proof that the adjudication was accurate. A denied claim is not proof that the service was nonpayable.
That's why providers need more than billing competence. They need adjudication literacy. Once you understand what the payer system is trying to accomplish, you can design claims that survive those checks instead of reacting after the payment variance appears.
The Step-by-Step Claim Adjudication Flow
The easiest way to understand the claim adjudication process is to think of it as a digital assembly line. Each claim moves through a sequence of gates. If it passes each gate cleanly, it stays in the fast lane. If it fails a check, it gets diverted into delay, rework, or manual review.
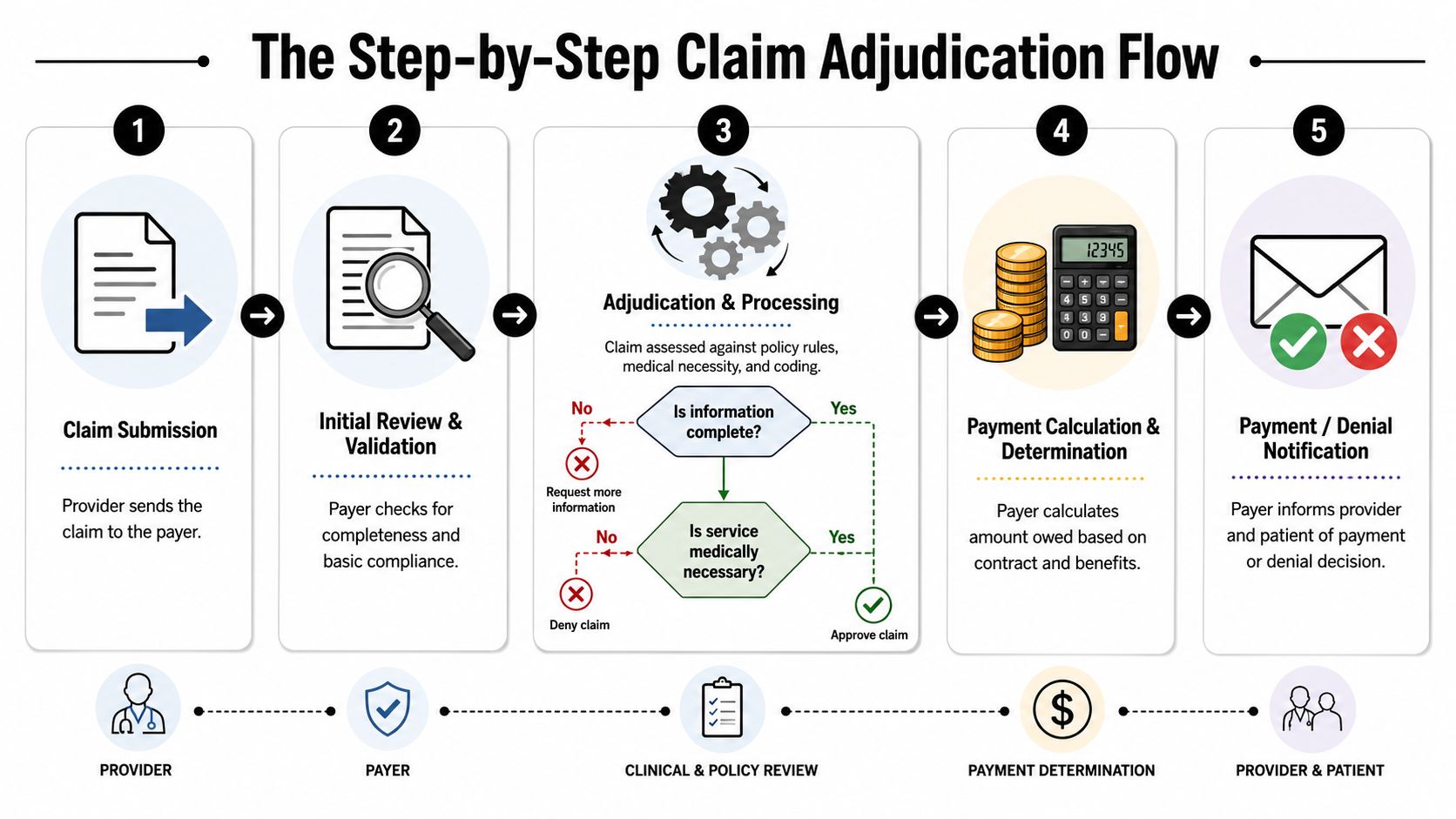
Step 1 through Step 2
The process starts when the provider submits the claim. Before the payer evaluates medical or financial merit, its system performs structural and intake checks. An industry overview from PCH Health on navigating healthcare claims adjudication notes that payer systems first run validation checks for duplicates, missing fields, eligibility, diagnosis and procedure-code consistency, and member identity matches before deciding whether to pay, reduce, deny, or route the claim for human review.
This stage is where a lot of avoidable failures begin. If the patient identifiers don't align, the service date doesn't line up with coverage, or the coding set creates an internal conflict, the claim may never reach the higher-value question of medical appropriateness. It fails on intake hygiene.
Step 3 through Step 4
If the claim clears validation, the payer's edits engine applies policy and payment logic. This can include benefit limits, authorization requirements, code-pair logic, coverage exclusions, bundling edits, and contract pricing methodology. The system then calculates the payable amount, member responsibility, and any reduction or denial outcome.
This is the phase where providers often underestimate the effect of upstream documentation and registration work. The adjudication engine is heavily rule-driven. It doesn't infer intent. It only sees the data elements and documentation trail it can validate.
A practical way to think about it is this:
- Clean intake data helps the claim enter the fast lane.
- Strong coding and documentation alignment helps it survive clinical and policy edits.
- Clear contract expectation mapping helps you spot whether the final paid amount is correct.
Auto-adjudication versus manual review
Most claims don't see a human examiner. The same PCH Health overview says about 85% of claims are handled by software without human review. That's why failed edits matter so much. Every avoidable exception pushes the claim out of an automated path and into a slower, more expensive lane.
Here's how those two paths differ in practice:
| Path | What usually triggers it | What it means for the provider |
|---|---|---|
| Auto-adjudication | Complete data, clean edits, standard policy fit | Faster disposition, but also faster denials if payer rules fire aggressively |
| Manual review | Missing information, unusual combinations, complex clinical or payment questions | Longer cycle time, more staff follow-up, higher chance of pends and documentation requests |
The fastest claim isn't the one submitted first. It's the one that gives the payer's system no reason to hesitate.
Final disposition
At the end of the flow, the payer issues one of a few outcomes:
- Paid as expected
- Paid with reductions
- Denied
- Pended for additional information
From an RCM perspective, that final status should never be the first time your team starts asking what happened. By then, the better question is whether your upstream workflow created a claim that was built to clear this assembly line, or built to fight its way through it.
Decoding Denial Root Causes and Payer Behaviors
Many teams still treat denials like isolated mistakes. One claim had a coding issue. Another needed authorization. Another hit medical necessity. That mindset keeps staff busy, but it doesn't give management control.
Denials are often patterned. The faster you start reading them as signals of payer behavior instead of random defects, the faster your denial strategy improves.

Faster processing can still mean worse outcomes
An established healthcare vendor says the industry average denial rate is 10% or higher, while its customers using automation report around 4%, according to MedVision Solutions on how claim adjudication works. The useful takeaway isn't that automation is automatically good. It's that process design changes results.
That same source makes a point many provider groups miss. Faster adjudication is not always better adjudication. It can mean faster rejections when claims are rule-edited early and aggressively.
So if a payer starts turning claims around quickly but your net collections weaken, speed may be hiding friction rather than reducing it.
Three denial buckets worth separating
Practice managers should sort denials into patterns that drive different responses.
Administrative breakdowns
These include coverage mismatches, missing identifiers, eligibility failures, coordination-of-benefits issues, and authorization gaps. They usually point back to front-end controls.
These are the easiest to prevent and the most frustrating to rework because they consume labor without adding reimbursement value.
Clinical validation disputes
These involve medical necessity, documentation sufficiency, level-of-service disagreement, and code-to-record mismatches. They often require chart-backed rebuttal rather than a simple corrected claim.
Coding quality and physician documentation discipline are paramount. If your clinicians document for care but not for payer scrutiny, the billing team inherits a weak record.
Payment integrity issues
These are the denials many groups under-detect. The claim may not deny outright. Instead, the payer reduces, downcodes, reprices, or pays below expectation. Staff may post the payment and move on because there is no loud denial event.
That's why teams need a denial framework that includes underpayments and questionable reductions, not just zero-pay outcomes. A structured healthcare denial management workflow should help your staff distinguish correction work from escalation work.
If the same payer keeps producing different denial language for the same operational problem, treat that as a payer-pattern issue first and a staff-error issue second.
What to watch for in payer behavior
Look for clusters, not anecdotes:
- Repeat edits by payer and service line
- Sharp increases in pends for documentation already submitted
- Frequent “not medically necessary” outcomes on clinically routine cases
- Consistent reductions on high-value codes or modifiers
- Remittance language that obscures the true reason for the variance
Teams get better results when they stop asking, “Why was this claim denied?” and start asking, “What rule, workflow failure, or payer pattern keeps producing this class of denial?”
That shift changes appeal quality, training priorities, and contract escalation strategy.
Essential KPIs for Monitoring Adjudication Performance
You can't manage the claim adjudication process from anecdotes. You need a dashboard that shows where claims break, how often they break, and whether the problem starts before submission or after payer review.
A KPI set should do two jobs at once. It should show internal process discipline and payer-side friction. If it only measures staff productivity, you'll miss underpayments. If it only measures denials, you'll miss the front-end defects causing them.
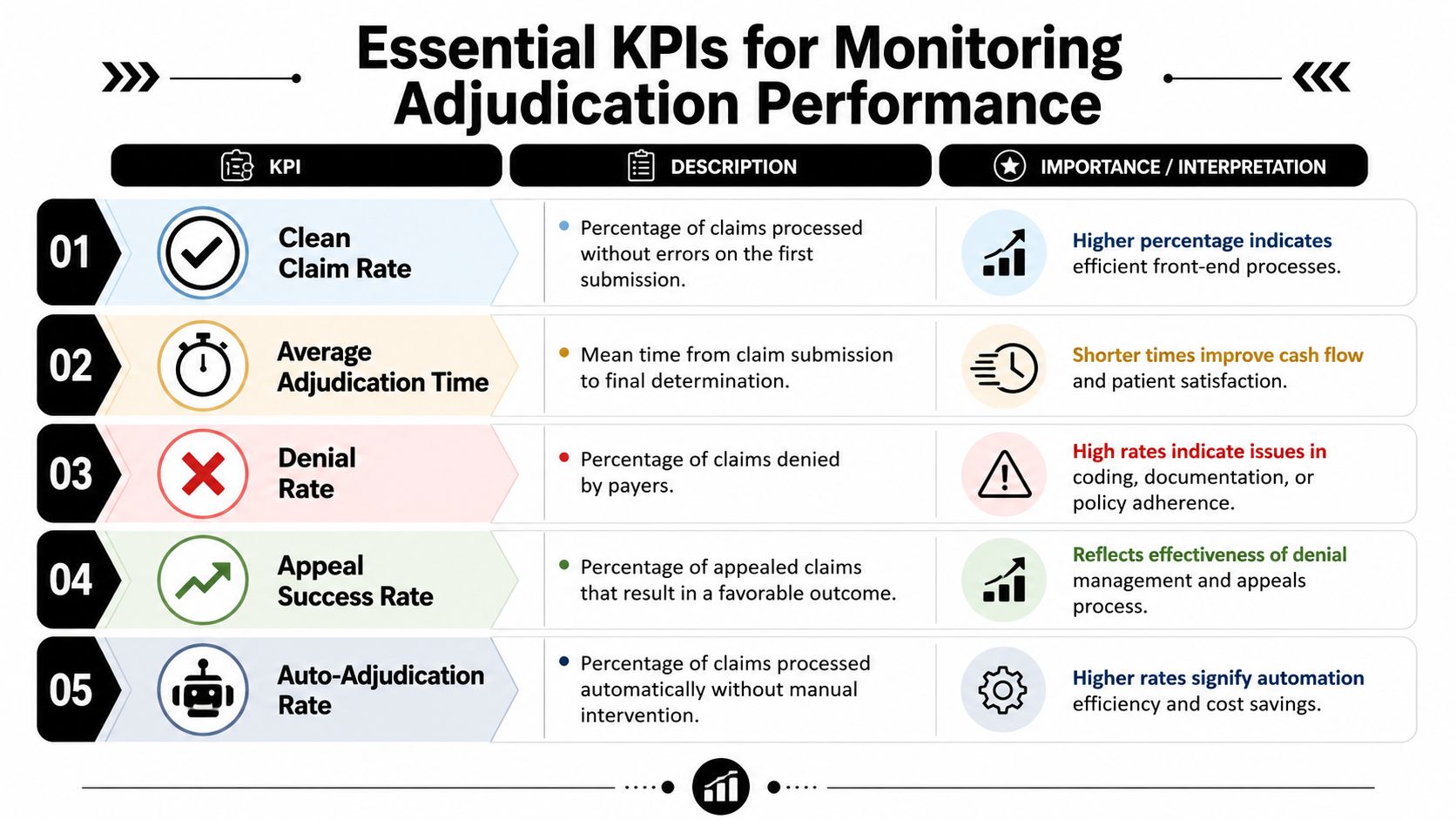
The core metrics that actually help
I'd keep the adjudication scorecard tight. Too many groups track everything and act on nothing.
| KPI | What it tells you | What a weak result usually means |
|---|---|---|
| Clean Claim Rate | How often claims go out without preventable defects | Front-end registration, eligibility, auth, or coding intake issues |
| First Pass Resolution Rate | How often claims resolve without rework | Claims are entering avoidable exception paths |
| Denial Rate by payer and reason | Where friction concentrates | Specific payer edit behavior or recurring process failures |
| Average adjudication time | How long cash is exposed to delay | Pends, manual review, document chasing, or payer lag |
| Net Collection Rate | Whether billed and allowed revenue converts into cash | Underpayments, write-off leakage, weak follow-up, or bad contract execution |
How to interpret the numbers together
No single metric tells the full story.
If Clean Claim Rate is soft and denial volume is high, you likely have upstream process problems. Focus on registration quality, eligibility verification, authorization capture, and coding edits before submission.
If clean claims look solid but net collections weaken, the issue may be downstream. Look for underpayments, contract variance, bundling behavior, or reductions that staff are accepting too easily.
If adjudication time rises without a corresponding increase in denial volume, your claims may be getting pended rather than denied. That usually means your team needs better documentation indexing, stronger work queues, or faster responses to payer requests.
A practical monitoring cadence
Most practice managers benefit from reviewing these KPIs at three levels:
- Daily operational view for exceptions, pends, and priority follow-up
- Weekly payer view for denial trends and turnaround patterns
- Monthly executive view for cash impact, variance, and escalation priorities
Operating advice: Don't just trend denial categories. Trend overturn categories too. If appeals repeatedly win on the same issue, that's a signal to redesign the original claim build and challenge payer behavior more directly.
What not to do
Avoid vanity reporting. A dashboard that says “denials are down” isn't enough if underpayments are up or payment variance is getting buried in adjustment codes.
The strongest KPI programs tie every metric to action. If a number moves, someone should know who owns it, what file sample to review, and whether the fix belongs in registration, coding, billing, contracting, or dispute escalation.
Winning Disputes Under the No Surprises Act
For organizations exposed to out-of-network payment disputes, the biggest mistake is treating IDR like a separate legal event that starts after a bad payment lands. It doesn't. The dispute is shaped much earlier, when your team decides what evidence to capture and preserve on the original claim.
That's why I push a single-continuum model. If a claim may later need open negotiation or federal arbitration, the intake, coding, documentation, and payment variance review all need to support that possibility from day one.
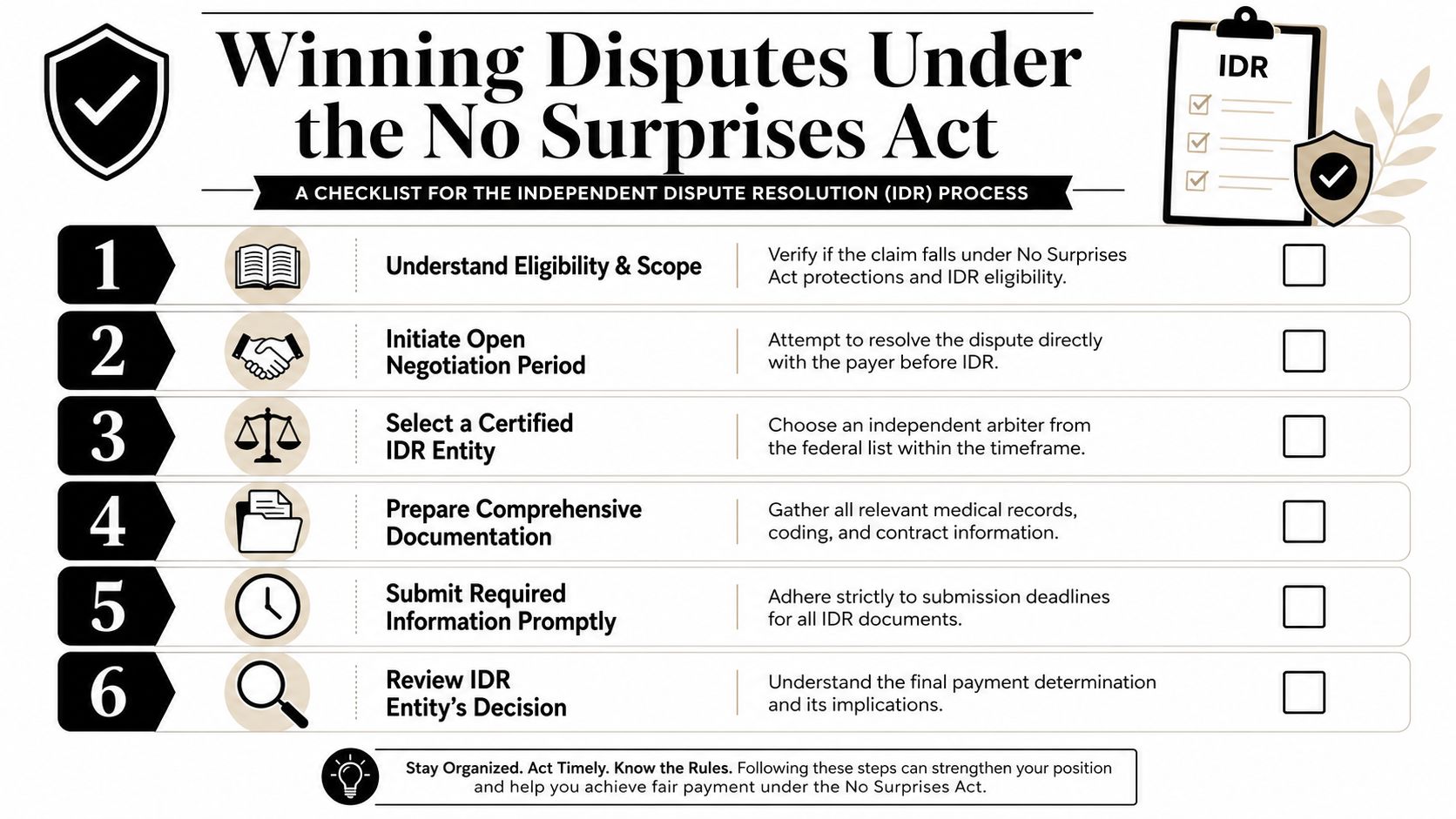
What dispute-ready actually means
A dispute-ready claim file usually includes more than the claim form and remittance. It should preserve the operational record that explains why the billed service was appropriate, how coverage and authorization were handled, what was submitted, what was paid, and why that payment appears inconsistent with the governing reimbursement framework.
For affected specialties, that often means building a complete package with:
- Patient and encounter support such as registration data, eligibility confirmation, and service context
- Clinical and coding support including records, physician documentation, code rationale, and modifier support where relevant
- Payment support such as the initial payer determination, remittance details, and internal variance analysis
- Dispute chronology that shows deadlines, open negotiation activity, correspondence, and preserved submissions
Why weak files lose even when the merits are good
A provider can be right on the substance and still lose their advantage because the file is incomplete, inconsistent, or poorly organized. Payers often benefit when providers can't reconstruct what happened after the fact.
That's why the handoff between RCM and dispute work matters so much. If your billing team corrects, rebills, appeals, and negotiates without preserving a clean timeline, your IDR position weakens.
The practical answer is to operationalize a linked workflow. Teams should know how RCM and IDR work together before the dispute starts, not during deadline pressure.
Build every potentially disputed claim file as if an independent reviewer will need to understand it quickly, with no institutional memory and no tolerance for missing support.
Where provider teams usually improve fastest
The most effective changes are often procedural, not dramatic:
- Preserve every payer-facing artifact rather than relying on portal history later.
- Standardize variance review so underpayments are identified consistently.
- Create specialty-specific evidence checklists because anesthesia, emergency care, imaging, and air transport don't all need the same support.
- Separate correction from contesting so staff know when to fix a provider-side defect and when to escalate a payer-side payment issue.
That discipline doesn't just help with federal disputes. It improves ordinary appeals too, because a well-built file shortens the time between identifying a variance and making a credible payment challenge.
How to Optimize Your Adjudication Outcomes
Margins disappear long before a denial is posted. Adjudication performance is shaped at intake, reinforced in coding and billing, and proven later if a payer cuts payment or forces a dispute. Teams that treat adjudication as one continuous process usually recover more revenue because they build claims to pay cleanly and defend cleanly.
Start with the parts of the workflow that create expensive downstream rework. Registration errors, weak authorization support, and plan mapping mistakes do more than delay payment. They also weaken your position if the account later moves into appeal, underpayment review, or IDR. A practice manager should be able to answer three questions at any time: where bad data enters the account, how fast the team catches it, and whether the correction is preserved in a way that supports a later challenge.
Tighten the front end first
The front end sets the ceiling on reimbursement.
Eligibility should be checked before the encounter and again when the date of service changes or coverage is uncertain. Authorization workflows should retain proof inside the account, not in someone's inbox or a portal screenshot that disappears later. Financial class and plan mapping controls should route claims correctly on the first pass, because a routing mistake often turns into a denial, a rebill cycle, and extra A/R days.
Those controls are operational, but the payoff is financial. Fewer preventable edits mean faster adjudication, fewer avoidable denials, and a cleaner record if the payer underpays.
Build coding and billing for scrutiny, not just submission
A clean claim file is not the same as a dispute-ready claim file. Payers may accept the format and still reduce the payment based on modifier logic, diagnosis combinations, policy edits, or contract interpretation. That is why coding teams need feedback tied to payer behavior, not just scrubber outcomes. If the same service pattern keeps drawing reductions, review the documentation and billing rule before staff send another corrected claim.
Billing teams also need separate decision paths:
| Workflow | Best use case |
|---|---|
| Correction path | Provider-side defect, missing data, or resubmission issue |
| Contest path | Payer reduction, denial pattern, underpayment, or unreasonable interpretation |
This distinction matters. Teams that send payer-side underpayments through a correction workflow lose time, reset filing clocks, and dilute the record needed for appeal or IDR.
Use analytics to direct human effort
Every variance does not deserve the same level of work. Staff time should go to claims where reimbursement risk, payer behavior, and recoverable dollars meet. That usually means repeat denial categories, partial payments that fall below expected reimbursement, slow-paying plans, and service lines with recurring policy edits.
Some organizations handle this with internal reporting and clearinghouse data. Others use payer intelligence platforms or firms like RevGuard, which links operational RCM with dispute enforcement by combining specialty-specific workflows, payer-behavior analytics, payment variance review, and No Surprises Act IDR support. The value is not software for its own sake. The value is keeping one record from claim build through payment review and, when needed, formal dispute.
What works
The tactics that hold up over time are straightforward:
- Standardize intake controls
- Audit denial and underpayment patterns by payer, service line, and code set
- Track payment variance, not just zero-pay denials
- Store documentation in a file structure that can support appeal or IDR without reconstruction
- Escalate repeat payer behavior as a pattern, not as isolated claim noise
What fails is a process built on memory. If reimbursement depends on a few experienced billers remembering payer quirks, collections slow down, training gets harder, and turnover exposes revenue.
The strongest adjudication outcomes come from dispute-readiness built upstream. Clean claims matter. Claims that are clean, well-supported, and organized for challenge recover more money, faster, and put the practice in a stronger position when payment disputes move beyond ordinary appeals.