
Your billing team is working denials every morning, your front desk is still chasing eligibility after the visit, and your physicians are asking the same question every month: why are collections lagging when volume hasn't collapsed?
That situation usually gets labeled as a billing problem. It isn't. It's a revenue system problem.
For specialty practices, ASCs, hospital service lines, and multi-site provider groups, the financial pressures are more pronounced now. Payers aren't just slow. They're procedural. They exploit registration errors, authorization gaps, coding inconsistencies, and weak follow-up discipline. In the No Surprises Act environment, that weakness carries downstream consequences. If your claim isn't built correctly on the front end, your negotiating position later, including payment disputes and IDR strategy, gets weaker.
Revenue cycle management outsourcing deserves a more serious discussion than it usually gets. This isn't about handing off statements and hoping cash shows up faster. It's about deciding whether your organization can still run a high-discipline, payer-ready, dispute-ready revenue cycle in-house.
The Tipping Point for Your Revenue Cycle
A specialty practice usually reaches the tipping point subtly.
It starts with a few payer edits that used to be manageable. Then prior authorization rules change. Then a coder leaves. Then a billing manager spends more time filling staffing gaps than managing performance. By the time leadership says, “We need help,” the practice already has a clogged A/R pipeline, inconsistent follow-up, and too many claims that were flawed before they ever hit the clearinghouse.
That's why I'm direct with clients about this decision. If your internal team can't reliably control intake accuracy, coverage verification, documentation alignment, coding consistency, and denial response, you don't have an RCM department. You have a patchwork.
When the old model stops working
Most struggling practices don't fail because people aren't trying hard enough. They fail because payer complexity has outgrown the operating model.
A front desk lead handles insurance verification one way. A scheduler handles it another way. Coders work from what physicians document, not what the payer will defend. Billing follows up after denial, not before claim submission. Then leadership reviews reports after the money is already delayed.
That's backwards.
Practical rule: If your team spends more time fixing claims after submission than preventing defects before submission, your revenue cycle is underbuilt.
The market has already moved in that direction. The healthcare RCM outsourcing market reached $32.0 billion in 2024 and is projected to grow to $108.9 billion by 2033, while a 2024 MGMA Stat poll found that 36% of medical practice leaders said they would outsource or automate part of revenue cycle management in 2025, with 50% saying they would not and 14% unsure, according to BillFlash's summary of the market and MGMA poll.
That matters for one reason. Outsourcing is no longer a rescue move for distressed groups. It's a standard operating decision.
What smart operators see earlier
The better-run groups usually make the decision before the pain becomes visible in month-end financials.
They look for signs like these:
- Escalating payer friction: Staff are spending more time deciphering rules than executing a stable workflow.
- Leadership drag: Revenue cycle managers are buried in staffing, escalations, and rework instead of process control.
- Specialty complexity: Procedures, modifiers, place-of-service distinctions, and payer-specific edits are too nuanced for a generalist billing model.
- NSA exposure: Underpayments and out-of-network disputes require evidence discipline that starts long before any arbitration file is opened.
If that sounds familiar, stop debating whether outsourcing is a philosophical fit. Ask the harder question. Can your current model protect reimbursement from first contact through final payment enforcement?
If the answer is no, you're already late.
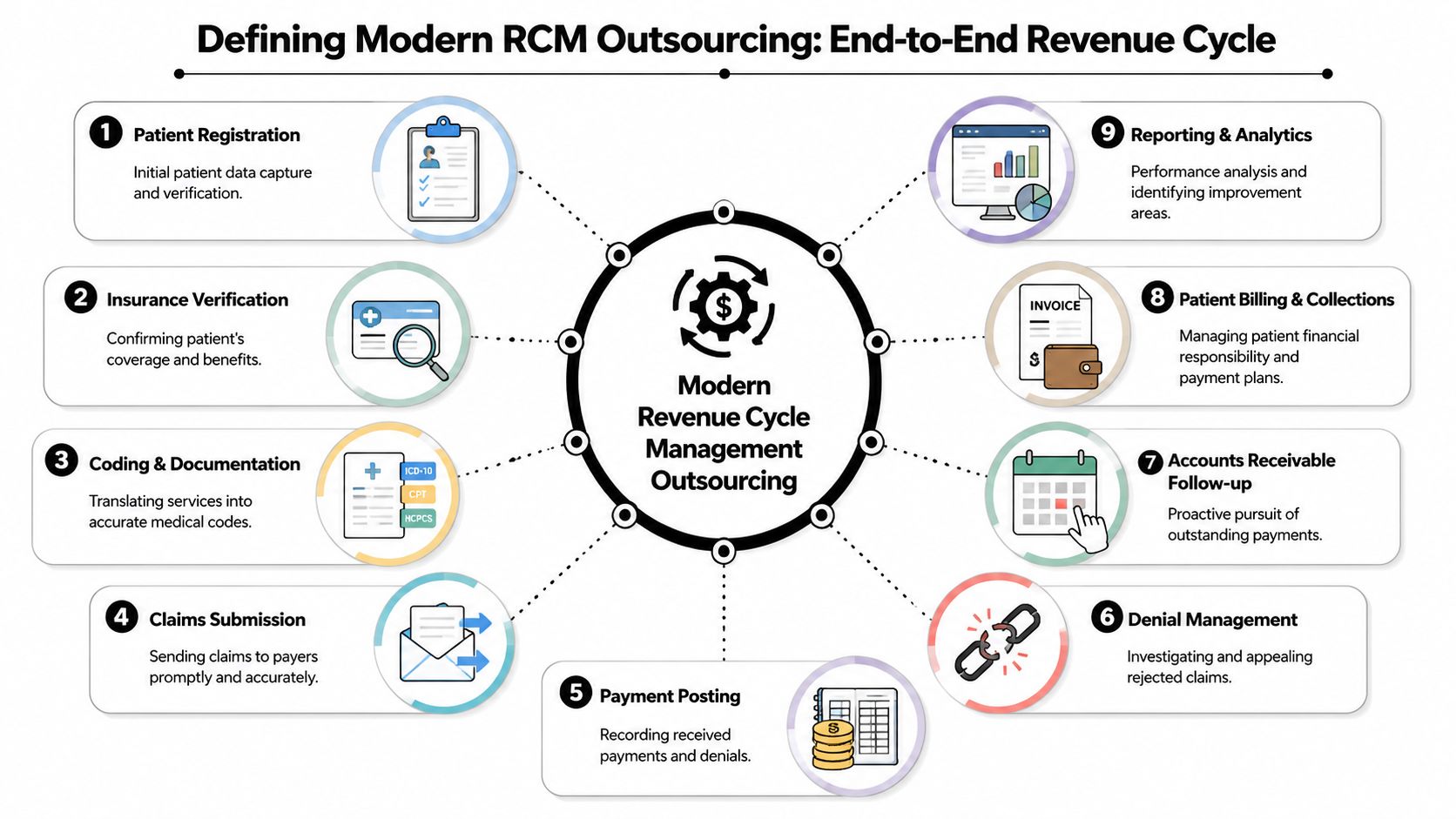
Defining Modern RCM Outsourcing
Modern revenue cycle management outsourcing is not “billing services.” That phrase is too small and too old.
A real outsourced RCM model covers the full financial lifecycle of an encounter, from patient access through final zero-balance resolution. It includes the operational work that prevents avoidable denials, the technical work that gets claims out cleanly, and the discipline required to post, appeal, collect, and escalate payment issues without dropping handoffs.
Here's the simplest analogy. Weak in-house RCM looks like disconnected workshops. Registration works in one room. Coding works in another. Billing works in another. Nobody owns throughput. Modern outsourced RCM should work like a production line. Each step feeds the next, defects are caught upstream, and performance is managed as one continuous system.
What the scope should include
At minimum, a modern model should touch all of these operating layers:
- Patient access controls: Registration accuracy, insurance capture, demographic validation, and financial responsibility setup.
- Coverage and authorization discipline: Eligibility checks, benefit verification, authorization workflow, and payer-rule matching before service or claim submission.
- Documentation and coding alignment: Chart review, coding logic, modifier use, and charge capture consistency.
- Claims workflow execution: Claim creation, scrubbing, submission, edit resolution, and file acceptance.
- Back-end cash work: Payment posting, denial management, A/R follow-up, patient billing, collections, and reporting.
- Decision support: Analytics that show where cash leakage starts, not just where it finally appears.
If a vendor only talks about claim submission and collections, that's not end-to-end. That's outsourced cleanup.
Who benefits most
The groups that benefit most from revenue cycle management outsourcing usually share one trait. Their reimbursement logic is more complicated than their internal infrastructure.
That includes:
- Specialty physician groups with payer-specific coding and modifier nuance.
- ASCs and outpatient platforms where throughput is high and mistakes repeat at scale.
- Hospitals and multi-site providers dealing with fragmented workflows across departments.
- Air ambulance and emergency-linked providers where payment enforcement matters as much as claim generation.
- Private equity-backed groups that need standardization across locations without building a giant internal back office.
A capable partner gives these organizations three things that are hard to maintain internally at the same time: specialized labor, process consistency, and technology-backed visibility. This is why groups look at firms offering revenue cycle management services. They want an operating system, not extra hands.
Outsourcing makes sense when your reimbursement complexity has become operationally heavier than your management bench.
What modern means in practice
A modern RCM partner should act less like a vendor and more like a disciplined production manager.
That means they should be able to answer practical questions without hiding behind dashboards:
| Revenue cycle area | What a serious partner should control |
|---|---|
| Intake | Demographic accuracy, insurance integrity, timely verification |
| Pre-claim | Authorization status, coding readiness, claim edits |
| Post-claim | Payment posting discipline, denial root cause tracking, appeal routing |
| Management | KPI visibility, payer trend analysis, accountability by work queue |
If they can't show how the process connects from intake to payment enforcement, they're selling labor. You need infrastructure.
Choosing Your RCM Outsourcing Model
Not every organization should outsource the same way. That's where many leadership teams get stuck. They assume the choice is all or nothing.
It isn't.
You have three practical models to choose from, and the right one depends on your operational maturity, specialty complexity, and tolerance for internal management overhead. The mistake is choosing based on comfort instead of choosing based on failure points.
The market is moving toward broader scope
Larger providers have already started leaning into fuller arrangements. According to Data Bridge's summary of healthcare RCM outsourcing market research, KLAS Research reported that the number of organizations signing new end-to-end outsourcing contracts nearly doubled since 2023, rising from 8 estimated new contracts to 14.
That trend makes sense. Once a provider sees that denials, A/R drag, and underpayments all trace back to upstream defects and fragmented ownership, partial fixes stop looking efficient.
RCM outsourcing models compared
| Model | Best For | Typical Scope | Level of Control |
|---|---|---|---|
| Full end-to-end outsourcing | Large specialty groups, hospitals, multi-site platforms, groups with chronic workflow breakdowns | Patient access, verification, coding support, claims, posting, denials, A/R follow-up, patient collections, analytics | Lower direct control over daily execution, higher control through governance and reporting |
| Hybrid or co-sourced model | Groups with a capable internal leader but weak capacity in certain functions | Shared ownership between internal staff and external team, often split by front-end, back-end, or payer class | Moderate control, requires strong role clarity |
| Specialty or component outsourcing | Practices with one acute pain point such as denials, aging A/R, coding backlog, or NSA/IDR work | Narrowly defined function with clear handoffs | Highest retained internal control, but also highest coordination burden |
Full end-to-end outsourcing
This is the right answer when the whole machine is unstable.
If your intake process is inconsistent, coding isn't standardized, denials are recurring, and no one trusts the dashboards, stop trying to preserve fragments of a broken model. Full outsourcing gives one operating partner responsibility for the entire cycle. That reduces handoff failure and puts one team on the hook for workflow discipline.
This model fits best when:
- You need standardization across sites
- Your internal leadership bandwidth is thin
- Payer complexity is too high for a fragmented team
- You want one governance structure instead of several disconnected vendors
The downside is obvious. You'll give up some direct day-to-day control. That's acceptable only if the contract, reporting, and oversight structure are tight.
Hybrid or co-sourced models
This is the best model for groups that still have some internal strengths worth keeping.
Maybe your patient access team is strong, but denials are a mess. Maybe your coding leadership is solid, but follow-up work is inconsistent. Maybe you want to retain physician-facing functions in-house while outsourcing the industrial parts of the cycle.
Hybrid works when leadership is disciplined enough to define ownership clearly. It fails when both sides assume the other side is handling the exception queue.
Keep hybrid models simple. If it takes a whiteboard and three meetings to explain who owns a denial, the design is already too complicated.
Specialty or component outsourcing
This model is often used by organizations that aren't ready for broad change but have one obvious leak they can't ignore.
Examples include:
- Denials management
- Legacy A/R recovery
- Coding support
- Patient collections
- No Surprises Act dispute and IDR support
There's nothing wrong with starting here. But be honest about the limitation. Component outsourcing treats symptoms well. It rarely rebuilds the whole revenue cycle. If your front end is still weak, specialized back-end help won't solve the underlying problem.
The right model is the one that matches the location of your operational failure. Not the one that feels least disruptive.
Evaluating the Business Benefits and Risks
Outsourcing RCM can improve financial control. It can also create a different set of management risks if you choose badly or govern loosely.
Both things are true.
The providers that get value from revenue cycle management outsourcing treat it like a controlled operating partnership. The providers that regret it usually treated it like a staffing swap.
Where the upside actually comes from
The biggest benefit isn't “someone else does billing.” The true gain comes from upstream discipline.
The most impactful control in RCM is front-end claim quality. A strong outsourcing partner integrates eligibility verification, prior authorization, and claim scrubbing into a single workflow, reducing rejections and accelerating reimbursement by coordinating EDI 837 generation, clearinghouse submission, and ERA/835 posting as one process, according to Premier NX's explanation of front-end RCM controls.
That matters because bad front-end work creates expensive back-end labor. A missing auth. A mismatched subscriber ID. A coding inconsistency. An eligibility error that should have been caught before the patient was seen. Every one of those defects turns into delayed cash, avoidable touches, and often preventable write-offs.
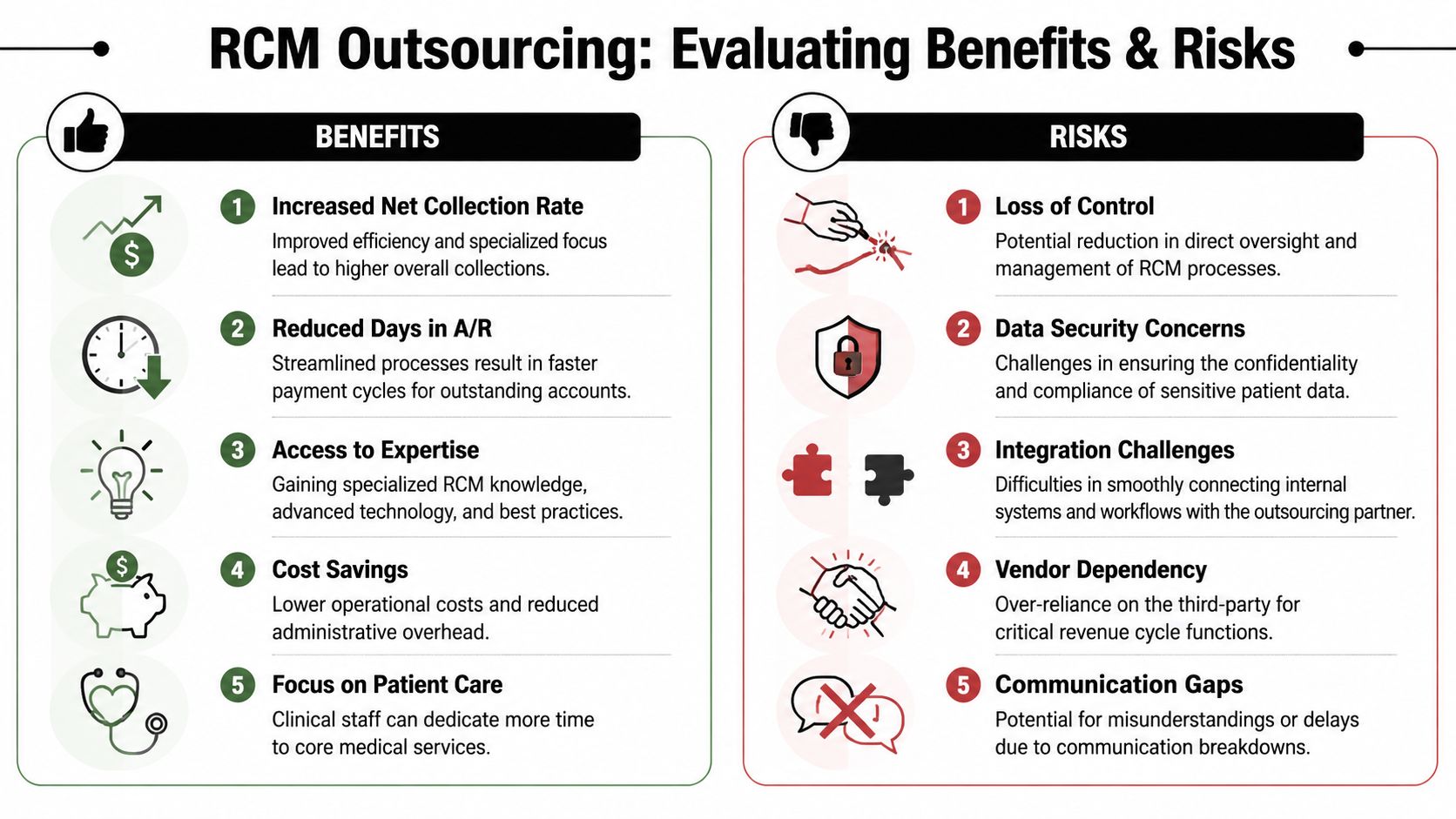
Benefits worth caring about
The useful benefits are operational, not cosmetic:
- Cleaner claims in the first pass: Better pre-submission controls reduce avoidable defects.
- Faster cash movement: Stronger workflow integration shortens the gap between service, submission, adjudication, and posting.
- Specialty-specific execution: Experienced teams know where payer edits, modifier issues, and documentation mismatches usually appear.
- More disciplined denial handling: Instead of chasing every denial the same way, better partners route and prioritize by root cause.
- Better management visibility: A good dashboard shows accountability by queue, payer, aging bucket, and denial class.
These aren't perks. They're the mechanics of revenue protection.
The risks are real too
You should worry about four things before you sign:
| Risk | What it looks like | How to mitigate it |
|---|---|---|
| Loss of control | The vendor runs a black box and reports after the fact | Require shared dashboards, queue-level visibility, and governance meetings |
| Vendor dependency | Critical know-how leaves with the partner | Preserve internal oversight roles and document workflows |
| Integration trouble | Data, systems, and work queues don't connect cleanly | Force implementation planning before contract signature |
| Communication gaps | Appeals stall, denials age, staff blame each other | Set response standards, escalation paths, and named owners |
I'd add a fifth risk that doesn't get enough attention. Misaligned incentives. If the vendor gets paid regardless of front-end quality, denial prevention won't get the attention it deserves.
Bad outsourcing doesn't remove chaos. It just moves chaos outside your org chart.
What disciplined buyers do differently
The smartest groups don't ask, “Will outsourcing help?”
They ask:
- Which part of our current cycle is structurally weak
- Can the partner prove control over that specific area
- What reporting will let us verify that control every month
That's the right lens. Not vendor personality. Not software demos. Not promises about “integrated workflows.”
You're buying execution. Make them prove they can run the line.
Cost ROI and No Surprises Act Implications
Most leadership teams evaluate outsourcing too narrowly. They compare vendor fees to internal payroll and call that an ROI analysis.
That's incomplete.
A serious evaluation has to include the cost of rework, delayed payment, management distraction, preventable denials, weak patient collections, and underpayments you never properly challenge. In the No Surprises Act environment, the last category matters much more than many groups admit.
How to think about cost
RCM outsourcing fees are usually structured around collections, scope, or a defined service bundle. The exact pricing model matters less than whether the economics align with the work you need.
If your issue is broad operational instability, a narrow low-fee vendor can be more expensive in practice because your internal team still carries the hidden labor and cleanup burden. If your issue is highly specialized payer disputes, a generalist billing vendor may look cheaper and still leave recoverable revenue untouched.
I tell clients to evaluate cost in three layers:
- Direct spend: What you pay the partner.
- Internal retained cost: Staff, oversight, IT coordination, and exception handling you still own.
- Revenue protection effect: Whether the model improves clean claims, payment speed, denial control, and underpayment recovery.
That third layer is where many deals either prove their value or fall apart.
Why the No Surprises Act changed the equation
The No Surprises Act made one thing obvious. Revenue cycle work doesn't end when the claim is submitted. In many specialties, it doesn't even end when the payer issues payment.
If a payer underpays an eligible out-of-network claim, the provider may need to defend reimbursement through a regulated dispute path. That means the RCM operation has to produce claims and documentation that are not only payable, but dispute-ready. Coding logic, medical necessity support, authorization context, and payer correspondence all become part of revenue enforcement.
That's why I don't separate RCM from NSA strategy anymore. A weak front end undermines the back end. If the claim file is sloppy, your later payment challenge gets weaker.
For organizations dealing with transport and emergency-related reimbursement, the issue is even sharper. The compliance and payment dynamics around No Surprises Act air ambulance disputes demand an RCM process that preserves evidence from the start, not after the payer has already set the terms of the fight.
What a partner must be able to do now
A modern partner should handle more than billing throughput.
They should be able to:
- Engineer clean, supportable claims with documentation and coding discipline
- Track payer behavior so recurring underpayment patterns are visible
- Preserve the evidence trail needed for NSA and IDR action
- Coordinate payment enforcement when ordinary follow-up won't resolve the issue
If your RCM partner stops at claim submission and payment posting, they're not built for the current payer environment.
This is why outsourcing can't be judged as a pure cost center anymore. In the right specialty, with the right payer mix, the partner is part operator and part enforcement engine. That's a different value proposition.
A Vetting Checklist for Selecting Your RCM Partner
Most RCM sales processes are designed to make vendors sound interchangeable. They all promise dashboards, expertise, automation, and better collections.
Ignore the pitch deck. Run due diligence like you're hiring someone to control a core asset, because that's exactly what you're doing.
Start with specialty fit
If you're an anesthesia group, orthopedic platform, ASC, radiology group, or emergency-linked provider, don't hire a generic medical billing company and hope they'll learn your claims on your dime.
Ask direct questions:
- Which specialties do they already support
- How do they handle specialty-specific coding and modifier logic
- Who manages payer-rule updates for your service mix
- What happens when clinical documentation doesn't support the billed charge
If the answers sound broad, polished, and nontechnical, keep moving.
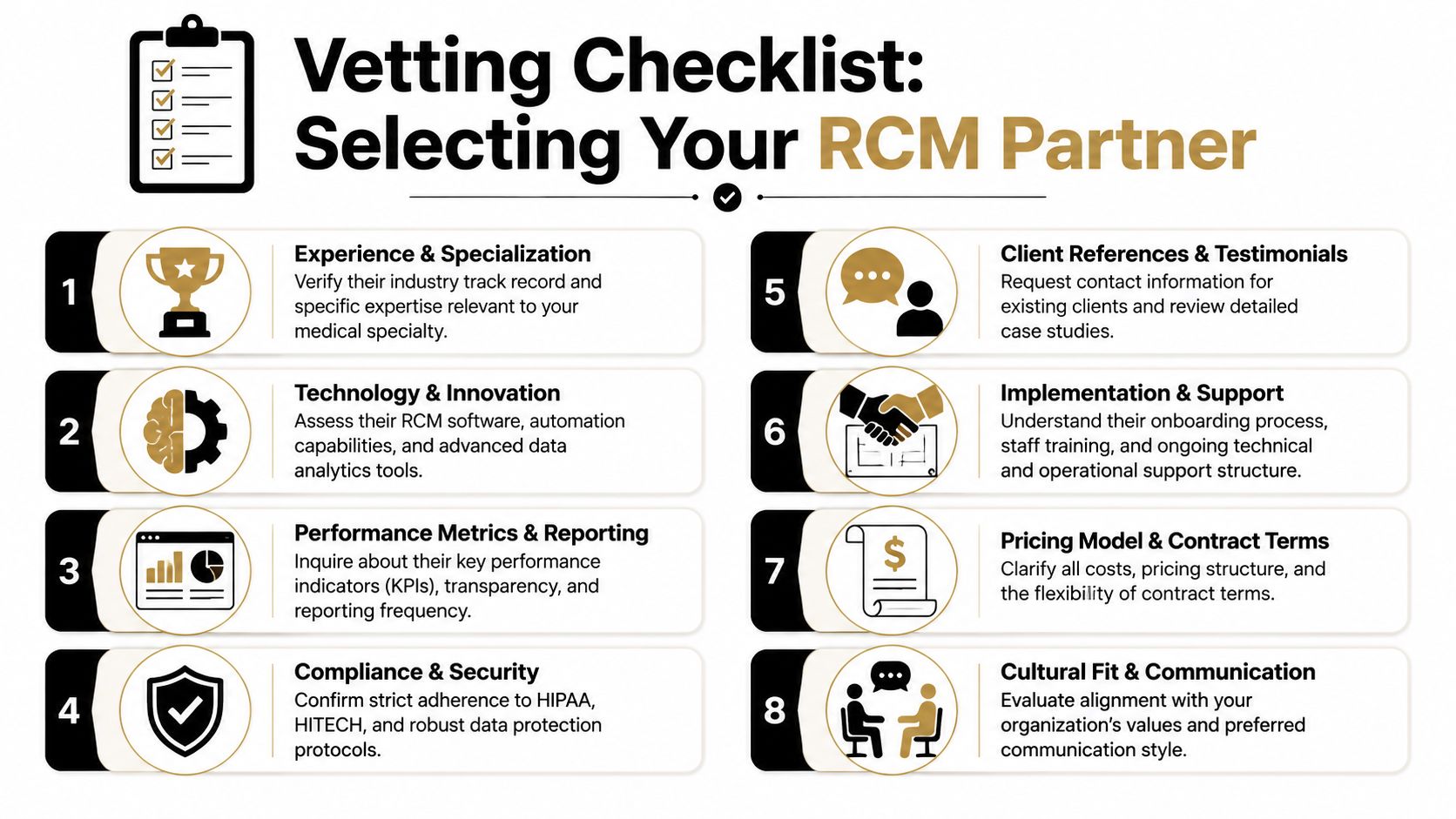
Demand transparency, not theater
A strong partner should be able to show you how work moves, who owns exceptions, what dashboards you'll see, and how issues get escalated.
Use this checklist during vendor review:
- Workflow visibility: Can they map the handoffs from registration through collections and dispute escalation?
- Technology clarity: Do they explain what is automated, what is manual, and where humans still review exceptions?
- Reporting discipline: Will you get queue-level reporting, denial categorization, payer trend analysis, and aging visibility?
- Compliance posture: Can they speak clearly about HIPAA handling, access controls, and operational safeguards?
- Implementation realism: Do they have a transition plan or just a promise that onboarding is easy?
- NSA capability: Can they explain how they support claims that may proceed into payment dispute processes?
- Governance model: Who attends operating reviews, and who has authority to resolve recurring problems?
- Account management: Will you have a real counterpart, such as a client success manager, or just a generic support channel?
Ask questions that expose weakness
Most bad vendor decisions happen because buyers ask soft questions.
Ask hard ones instead:
| Ask this | Why it matters |
|---|---|
| Show me a sample monthly operating report | It reveals whether they manage performance or just summarize activity |
| Walk me through a denied claim from intake to resolution | It exposes process depth and handoff quality |
| What do you require from our staff weekly | It shows the real operational burden you'll keep |
| What happens if performance stalls | It tests whether governance exists beyond contract signature |
The right vendor won't get defensive when you ask operational questions. They'll get specific.
Watch for red flags early
Walk away if you see any of these:
- Black-box reporting
- Vague explanations of staffing location or oversight
- No clear specialty expertise
- No structured NSA or underpayment response path
- A contract that protects fees better than outcomes
A good partner should make your revenue cycle more understandable, not less.
Ensuring a Smooth Transition and Long-Term Success
A signed contract doesn't stabilize the revenue cycle. Execution does.
Many groups often stumble here. They spend months selecting a partner and almost no time designing the transition, governance, and performance management that will determine whether the deal works.
For specialty and high-volume providers, outsourcing is often structured as a long-duration production system, with contracts of five years or more, embedding analytics, KPI benchmarking, and denial-prevention controls directly into the cycle, according to MGMA's discussion of outsourcing partnerships and hospital-based arrangements.
That long horizon is exactly why implementation discipline matters. You're not hiring temporary help. You're redesigning how money moves through the practice.
Get the transition sequence right
A smooth transition usually follows a practical order:
Current-state review
Map existing workflows, payer pain points, unresolved A/R issues, and staff dependencies before anything moves.Data and system preparation
Confirm access, interfaces, work queues, file flows, and reporting requirements. Don't let this become an IT afterthought.Workflow redesign
Decide how registration, auth, coding review, claims edits, denials, and patient collections will be handled in the new model.Staff alignment
Your internal team needs clear role definitions. Confusion during transition creates duplicate work and missed work at the same time.Stabilization period
Expect a period where defects surface. The point isn't to avoid all friction. The point is to catch and fix issues quickly.
Build a management system, not just meetings
After go-live, leadership should track a small set of operational KPIs on a shared dashboard. Not twenty-five. Not vanity metrics. The handful that reveal whether the line is healthy.
Focus on these:
- Clean claim rate: Are claims getting out correctly the first time?
- Denial rate: Are defects being prevented or instead appealed later?
- A/R aging: Is cash moving through the cycle or stalling in predictable buckets?
- Net collection performance: Are allowable dollars turning into collected dollars consistently?
- Authorization and eligibility exception trends: Are front-end controls tightening over time?
- Payer-specific failure patterns: Which plans create the most friction, and where exactly?
These metrics should lead to action. If a payer's edits spike, someone should own the fix. If one location has weaker registration accuracy, that should trigger retraining. If denials cluster around one procedure family, coding review should change.
Hold the partner accountable the right way
Monthly reviews are necessary. They're not sufficient.
You also need:
- Named owners on both sides
- A documented escalation path
- Written action plans for recurring issues
- A method for separating system defects from one-off exceptions
The best outsourcing relationships feel operational, not ceremonial. Problems are identified early, root causes are assigned, and the dashboard gets used to drive changes in workflow.
That's what long-term success looks like. Not “good communication.” Not “collaboration.” Actual control.
If your practice needs an RCM model that connects clean-claim discipline with No Surprises Act payment enforcement, RevGuard is one option to evaluate. The firm combines specialty-specific revenue cycle management with IDR and underpayment recovery workflows, which is especially relevant for groups that need both operational execution and post-adjudication enforcement.