
ClinicMind reports that 80% of medical bills contain at least one error, and 30% of insurance claims are denied on first submission. That should change how specialty practices think about medical billing audits.
If most bills carry some defect and a large share of claims fail on first pass, then audits aren't a back-office exercise for compliance binders. They're a revenue protection system. They identify where documentation breaks, where coding drifts, where eligibility controls fail, and where payer adjudication erodes value from otherwise valid claims.
In specialty settings, that's the difference between a manageable denial queue and a chronic margin problem. It also shapes what happens later if payment disputes escalate. A claim that was never audit-tested is usually weak in all the places that matter most: support for medical necessity, modifier logic, benefit verification, and payment variance documentation.
From Compliance Chore to Revenue Strategy
Most organizations still treat medical billing audits as a reaction. A payer asks questions. Compliance wants a sample review. Leadership sees denial volume rising and requests a spot check. That mindset is too narrow.
A strong audit program starts much earlier. It reviews the claim before bad habits become denial patterns and before underpayments become accepted write-offs. For specialty groups, the financial value isn't limited to avoiding takebacks. The bigger win is finding leakage that nobody sees when teams only monitor posted cash and gross charges.
Why the old framing fails
A compliance-only audit usually asks one question: was the claim billable? Revenue strategy asks a harder set of questions:
- Was the patient eligible: Did the front-end team verify active coverage and benefits accurately enough to prevent downstream denials?
- Was the chart defensible: Does the documentation support the diagnosis, procedure selection, and level of service?
- Was the claim built correctly: Were ICD, CPT, HCPCS, and modifier choices aligned with payer rules?
- Was the payment correct: Did the remittance reflect what the payer owed under policy, contract, or dispute posture?
Those are different jobs. A compliance lens catches risk. A revenue lens catches risk and missed payment.
For many practices, the practical shift starts when leadership stops asking, "Did we pass the audit?" and starts asking, "What part of the revenue cycle created this error, and how often is it happening?"
What effective programs do differently
Teams that get value from medical billing audits usually build them into routine operations, not annual cleanup. They tie findings to workflow owners and financial outcomes. They also connect audit results to front-end controls, coding edits, and remittance review instead of treating the chart as the whole story.
Practical rule: If your audit findings don't change registration scripts, documentation habits, claim edits, or payment review workflows, you ran a report, not an audit program.
That also changes how practices think about audit readiness. It isn't just about being prepared for outside scrutiny. It's about engineering cleaner claims from the start. If you need a broader view of how those controls fit into payer-facing requirements, this overview of medical billing compliance is a useful companion.
The Six Essential Types of Medical Billing Audits
Not all medical billing audits answer the same question. Some are routine maintenance. Some are forensic. Some happen before the claim leaves your system. Others happen after the payer has already acted on it.
A useful analogy is vehicle inspection. An internal audit is like your own maintenance check. An external audit is a third-party inspection. A prospective audit is what you do before driving onto the highway. A retrospective audit is what you do after the warning light has already turned on.
Comparison of Medical Billing Audit Types
| Audit Type | Performed By | Timing | Primary Goal | Example Scope |
|---|---|---|---|---|
| Internal | Practice or health system staff | On a routine schedule or targeted basis | Find operational errors early and improve workflows | Sample review by specialty, provider, payer, or location |
| External | Independent outside reviewer | Periodic or event-driven | Get an objective assessment and validate internal assumptions | Broader review of billing patterns, controls, and compliance risk |
| Payer | Health plan or payer representative | After submission, payment, or pattern detection | Verify billing accuracy and support payment decisions or recoupment | Focus on documentation, medical necessity, modifiers, or service frequency |
| Prospective | Internal coding, audit, or revenue integrity staff | Before claim submission | Prevent denials and weak claims before they go out | Pre-bill review of high-risk claims, new providers, or high-variability services |
| Retrospective | Internal or external reviewer | After claim submission or adjudication | Identify root causes, overpayments, underpayments, and repeat failure points | Post-payment review of denials, payment variance, and coding trends |
| Compliance | Compliance, legal, audit, or revenue integrity teams | Ongoing or issue-based | Test adherence to payer and regulatory expectations | Documentation support, coding accuracy, modifier use, and billing policy alignment |
How to choose the right audit type
The mistake many practices make is choosing one audit format and applying it to every problem. That rarely works.
A few examples:
- Use internal audits when denial trends are creeping up and you need a fast read on where defects originate.
- Use external audits when leadership needs an unbiased view, or when internal staff may be too close to the workflow to see persistent problems.
- Use payer audits as signals rather than isolated events. If one payer reviews a service line, assume your own controls need testing before others do the same.
- Use prospective audits for claims that are expensive to get wrong, such as specialty procedures, facility-based billing, or services with frequent modifier disputes.
- Use retrospective audits when posted payments don't match expectations and the issue may involve underpayment, downcoding, or silent contract variance.
- Use compliance audits when the pattern suggests broader exposure, especially if documentation support and coding logic are drifting in tandem.
What works and what doesn't
What works is matching the audit type to the operational question.
What doesn't work is ordering a generic chart review and calling it a revenue integrity strategy. If the actual issue is remittance variance, a documentation-only review will miss it. If the issue is front-end eligibility error, a coder re-education plan won't solve it.
For practices building a more mature program, coding, auditing, and compliance support matters most when it ties chart findings to claim edits and payer outcomes, not when it sits in a silo.
Common Audit Triggers and Financial Risk Indicators
Most providers assume audits start because someone made a blatant billing mistake. Sometimes that's true. More often, auditors arrive because the billing pattern itself stands out.
CareBiller notes that the risk isn't just the audit itself, but how it originates and escalates. Audits are often driven by aberrant billing patterns and comparative outlier detection, and the scope can widen significantly if auditors identify a pattern that can be interpreted as systemic rather than isolated. That's the operational reality specialty practices need to plan for.
The patterns that draw attention
Single-claim mistakes matter, but repeated behavior matters more. Payers and other auditors don't need every claim to be wrong. They need enough repeat variance to suspect a system issue.
Common risk indicators include:
- Outlier coding frequency: One provider, site, or specialty bills certain code combinations or levels of service at a rate that appears inconsistent with peers.
- Modifier concentration: A practice relies heavily on modifiers that materially affect payment and doesn't consistently support them in the chart.
- Complaint-driven scrutiny: Patient complaints or repeated payer inquiries push a claim pattern into a broader review.
- Documentation mismatch: The note supports some service, but not the service that was billed, or not at the level billed.
- Medical necessity disputes: The diagnosis, ordering logic, or clinical narrative doesn't align with payer expectations.
- Repeated eligibility failures: Coverage was assumed, not verified, and billing staff pushed the claim forward anyway.
In higher-variability specialties, these signals can be even more sensitive because payer benchmark models often compare service mix, utilization patterns, and coding behavior against peers.
Why small errors become systemic risk
Leaders often underestimate how escalation happens. A few recurring registration defects can create a consistent denial class. A recurring modifier error can produce a payer profile that suggests misuse, even if the underlying care was appropriate. A weak authorization process can create the appearance of careless billing controls.
A payer doesn't need to see intent to expand review. Repetition alone can justify broader scrutiny.
That is why front-end discipline matters so much. Specialty practices often focus on coding after the encounter, but a surprising amount of audit exposure starts before the patient is seen. Weak medical eligibility verification creates avoidable denials, inconsistent coverage assumptions, and downstream appeal weakness.
Specialty-specific pressure points
Not every service line gets flagged the same way. Anesthesia, imaging, surgery centers, emergency services, and hospital-based departments all carry different vulnerability points.
For example:
- Facility-based services often face modifier and adjudication complexity.
- High-acuity specialties face more medical necessity scrutiny because documentation must justify intensity and timing.
- Services with wide reimbursement variance face underpayment risk even when the underlying claim is clean.
- Multi-location groups often trigger pattern concerns because workflow inconsistency creates visible variation across providers and sites.
The practical takeaway is simple. Audit triggers are rarely random. They usually reflect a detectable pattern that already existed in your data before anyone asked for records.
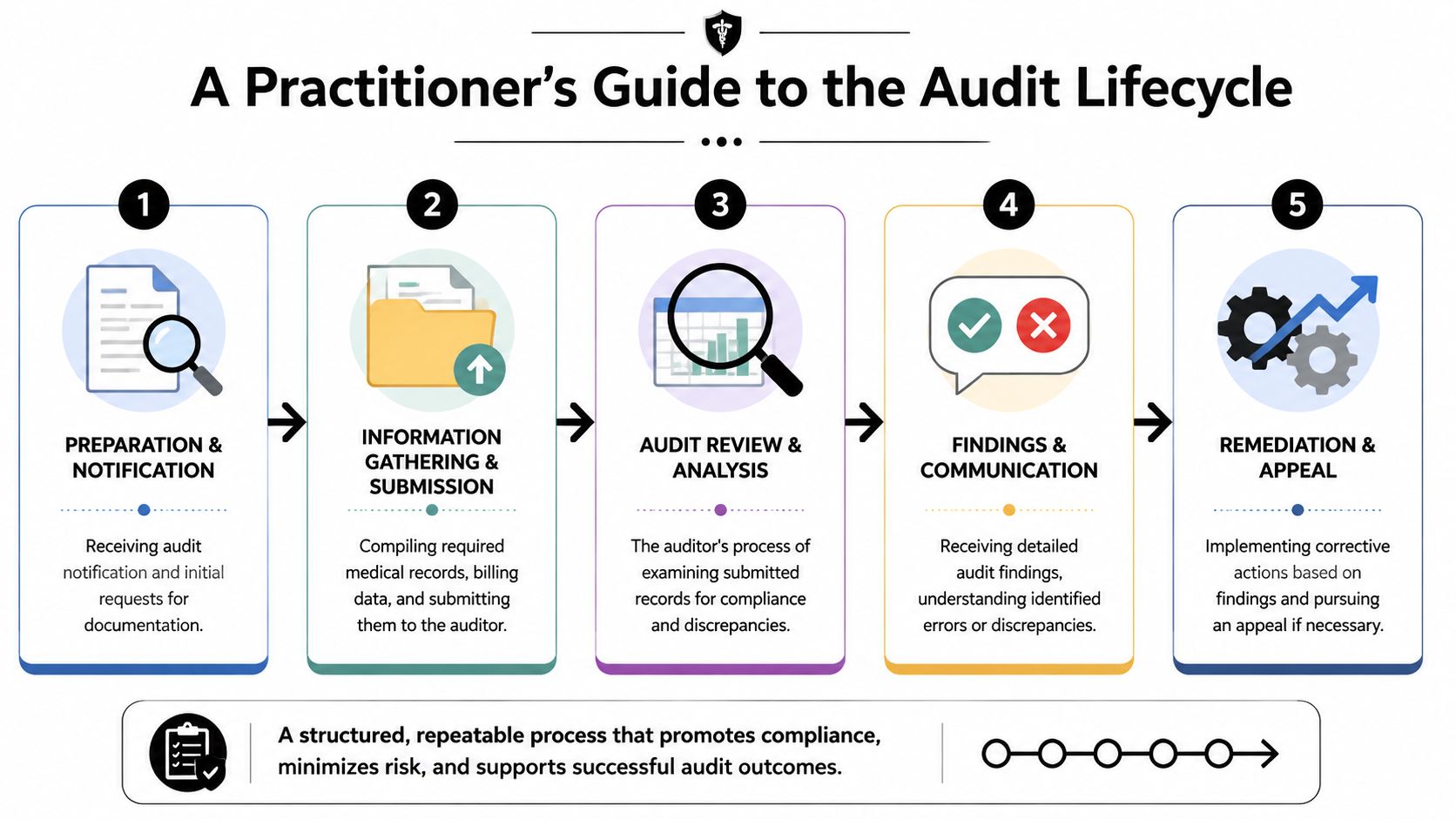
A Practitioner's Guide to the Audit Lifecycle
A workable audit program has to run like an operating process, not a one-time event. The basic lifecycle is consistent even when the scope changes. Planning comes first. Then data collection. Then chart and claim review. Then reporting. Then remediation and follow-up.
That discipline matters more today because the CMS Recovery Audit Contractor program was made permanent in 2010, marking a policy shift toward continuous post-payment review. Audit readiness isn't occasional anymore. It's part of modern revenue cycle management.
Step 1 through Step 2
The first phase is planning and scope definition. Decide whether you're testing a payer issue, a specialty line, a provider pattern, a denial category, or a payment variance question. Scope that is too broad creates noise. Scope that is too narrow hides repeat behavior.
The second phase is data collection and sampling. Pull records from the EHR, practice management system, claims history, payer remittances, and any relevant authorization or eligibility documentation. If you're auditing a specialty line, include enough variation to see patterns across providers, locations, and payer classes.
A solid planning checklist usually includes:
- Objective selection: Are you testing compliance exposure, denial root causes, underpayments, or all three?
- Data source alignment: Can you match the chart, coded claim, submitted claim, and remittance?
- Ownership assignment: Who validates findings and who implements fixes?
- Escalation criteria: What level of repeat error triggers a broader review?
Step 3 through Step 4
The third phase is chart review and analysis. Many audits lose value in this phase because reviewers stop at coding accuracy. That isn't enough. Compare the encounter record to code assignment, modifier selection, claim edits, and final adjudication. The point is to see where leakage entered the workflow.
The fourth phase is reporting and findings communication. Keep the report operational. A good report doesn't just list errors. It links each finding to a root cause, a workflow owner, and a financial consequence. If a denial category ties back to registration, say so. If underpayment appears payer-specific, isolate it clearly.
Field note: The best audit reports are uncomfortable in a useful way. They name where the process failed and who has to change it.
Step 5 and the follow-up discipline
The fifth phase is remediation and follow-up audits. Here, the program either becomes useful or dies in a shared folder. Corrective actions should be specific enough to change behavior.
Examples of effective follow-up actions include:
- Documentation fixes: Update specialty-specific templates and physician prompts where charts repeatedly fail to support billed services.
- Coding controls: Add targeted edits for known modifier or bundling risks.
- Front-end changes: Tighten benefit verification and authorization workflows when denials originate before the claim is coded.
- Payer response strategy: Track recurring payment variance by payer and service type so the team can challenge patterns, not just individual claims.
Then re-audit. If the same issue appears again, the original correction didn't reach the actual cause.
What seasoned teams avoid
Experienced revenue cycle teams avoid three predictable mistakes:
- They don't audit in isolation. Coding, front-end operations, denial management, and payment posting all have to be visible.
- They don't stop at findings. Every finding needs an owner, a due date, and a retest.
- They don't confuse activity with control. Reviewing charts without changing workflows creates the appearance of diligence without reducing risk.
Translating Audit Data into Actionable KPIs
An audit report becomes valuable when leadership can use it to decide where to intervene. That's why the strongest medical billing audits don't end with error narratives. They convert findings into operating metrics.
The KPI layer that actually matters
Too many dashboards track only lagging indicators. Total charges. Total collections. Days in A/R. Those matter, but they don't tell you where claims are weakening.
Audit-derived KPIs are more useful because they point to a root cause. In practice, the most actionable ones often include:
- Denial rate by payer and service line: Shows where rules, documentation, or front-end controls are misaligned.
- Code-level error frequency: Reveals whether mistakes cluster around specific CPT, HCPCS, diagnosis combinations, or modifiers.
- Underpayment rate or payment variance: Flags situations where the claim was accepted but the reimbursement wasn't fully aligned with expectations.
- Appeal overturn rate: Tests whether your original claim package and supporting documentation are strong enough to reverse payer decisions.
Build a closed loop, not a static dashboard
The workflow should move in a loop:
| Audit Output | KPI Created | Operational Response |
|---|---|---|
| Documentation variance | Code-level error trend | Update provider templates and coding review rules |
| Eligibility mismatch | Denial trend by reason and payer | Tighten front-end verification and authorization checks |
| Modifier misuse | Error frequency by modifier | Add claim edits and specialty retraining |
| Payment variance | Underpayment tracking by payer | Escalate recurring discrepancies for recovery review |
Not every error deserves the same response: A low-frequency issue with low financial effect may only need monitoring. A recurring issue tied to denials or underpayments needs immediate workflow redesign.
What leaders should ask every month
A productive KPI review isn't a finance-only meeting. Revenue cycle, coding, compliance, and operational leaders all need to see the same facts.
Ask questions like:
- Where are repeat defects starting?
- Which payer patterns are costing us the most effort or reimbursement?
- Did the last remediation step change the KPI we targeted?
- Are we looking at isolated claims, or are we seeing a process pattern?
If a metric doesn't point to a workflow owner and a corrective action, it isn't helping the audit program.
The point isn't to create more reporting. It's to make audit intelligence usable enough that teams can prevent the next round of avoidable leakage.
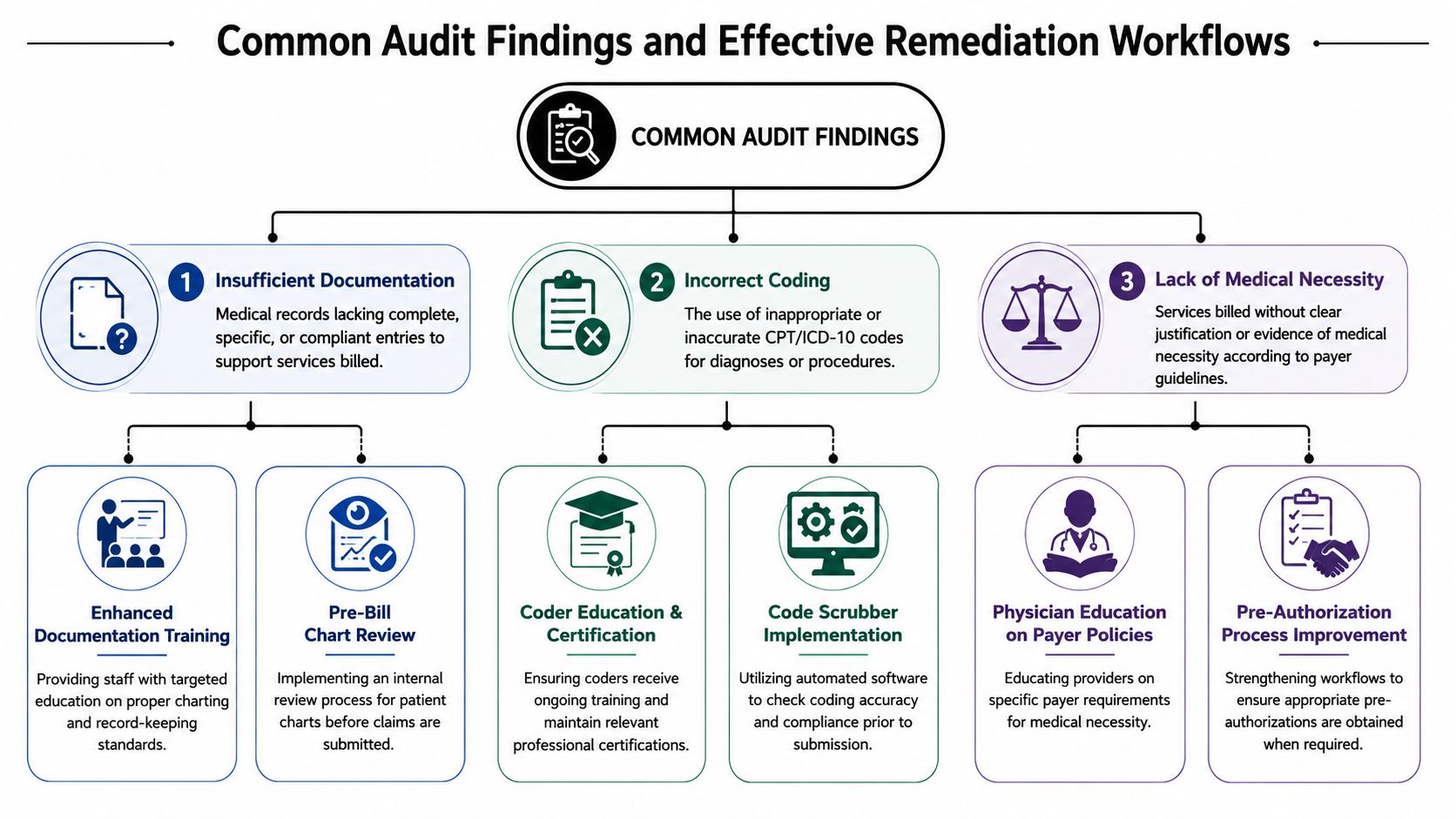
Common Findings and Effective Remediation Workflows
Most audit findings aren't exotic. They're familiar problems that survived because each team only saw one piece of the chain. That's why high-value medical billing audits look across eligibility, clinical documentation, code assignment, and remittance rather than stopping at a single claim view, as described by CBS Medical Billing's overview of end-to-end medical billing audit review.
Three findings that keep showing up
Start with insufficient documentation. The service may have been appropriate, but the record doesn't clearly support the billed diagnosis, intensity, or modifier logic. That creates denials, downcoding, and weak appeal posture.
Then there's incorrect coding or unbundling logic. Sometimes the problem is pure code selection. Other times the code itself is defensible, but the combination of codes, modifiers, or edit overrides creates risk.
The third recurring issue is medical necessity mismatch. The payer's policy expects a tighter link between diagnosis, order, service rationale, and chart narrative than what the record shows.
What effective remediation looks like
Weak remediation sounds like this: "educate staff."
Useful remediation sounds like this:
- For documentation gaps: Revise specialty templates, add required chart prompts, and have a reviewer perform a short pre-bill check on similar claims until support rates stabilize.
- For coding errors: Update edit logic in the claim scrubber, retrain coders on the exact code family or modifier issue involved, and run a focused follow-up sample on the same service type.
- For medical necessity disputes: Build payer-specific reference guidance for ordering and rendering clinicians, then require stronger support before claim release on services with repeated denials.
A good workflow also assigns ownership. If the problem starts in provider notes, coding can't own the entire fix. If the issue is eligibility or authorization, no amount of coder education will correct it.
A before and after pattern
Consider a common specialty scenario. A claim is denied for lack of support. The coding team reviews it and confirms the code set looks reasonable. The appeal still fails because the record doesn't clearly state why the service met payer expectations.
The failed approach is to resend the same documents with a short note. The effective approach is to map the miss precisely:
- Locate the break: Was the service clinically appropriate but poorly documented, or was the wrong payer rule applied?
- Patch the workflow: Add a provider prompt, a coder hold rule, or an authorization verification step.
- Retest the class: Review a new sample from the same service category to confirm the error has declined.
Strong remediation changes the next claim before it changes the next report.
That is the difference between an audit that archives findings and one that prevents repeat revenue leakage.
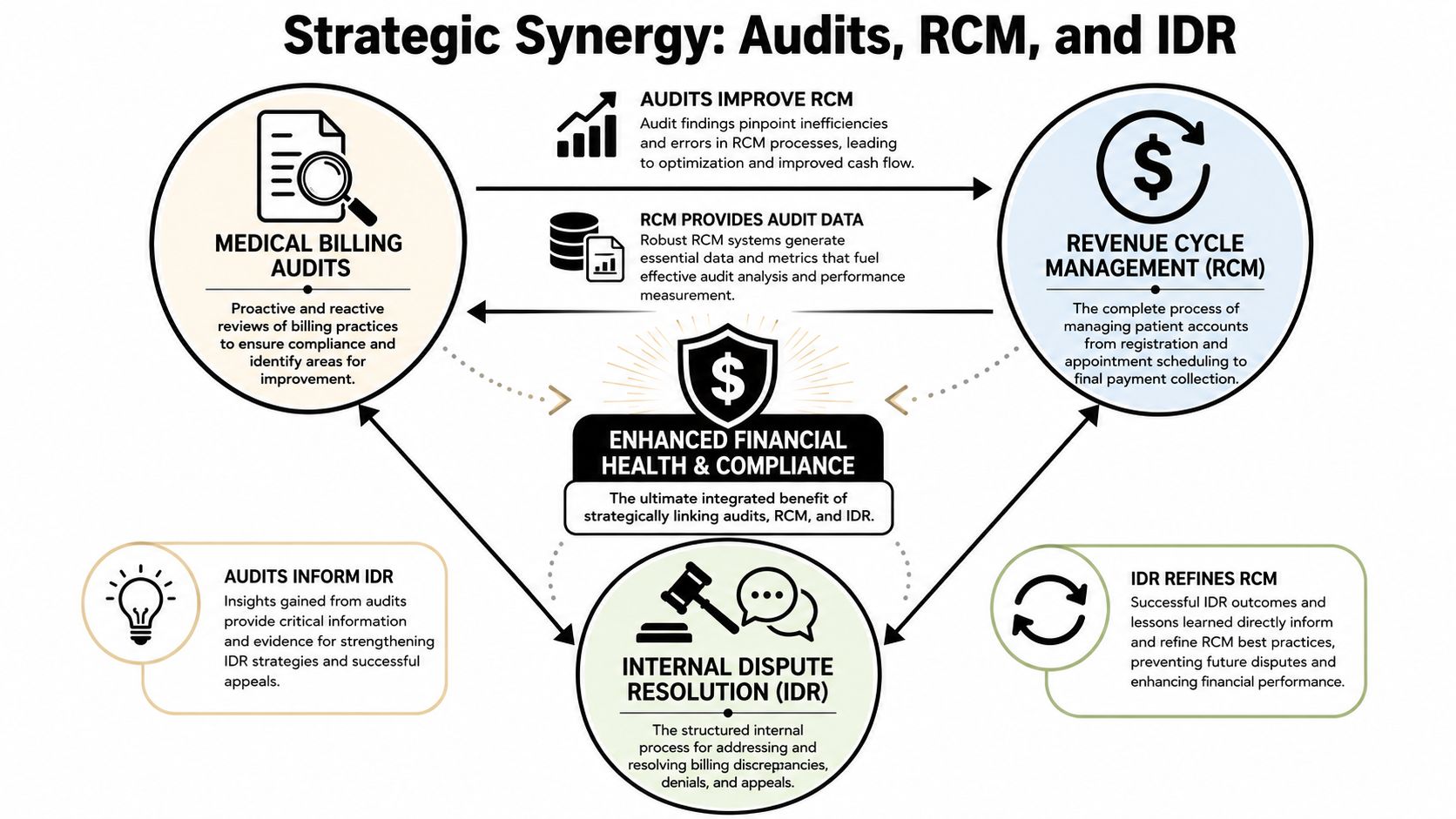
The Strategic Link Between Audits RCM and IDR
The most useful reason to invest in medical billing audits isn't just to reduce exposure. It's to make your claims stronger in the payer environment you're already operating in.
Specialty practices don't just face denials. They face downcoding, underpayments, delayed adjudication, and disputes over medical necessity or service structure. An audit program gives you the raw material to challenge those outcomes effectively because it tells you where the claim is strong, where the payer pattern is recurring, and what evidence should have been assembled at the outset.
Audit discipline creates dispute-ready claims
A dispute-ready claim usually has four qualities:
- The front-end record is clean: Eligibility, benefits, and authorization logic are documented well enough to survive scrutiny.
- The chart supports the service clearly: The clinical narrative aligns with code selection and medical necessity.
- The billing logic is defensible: Code combinations, modifiers, and edits are consistent with the service rendered.
- The payment variance is documented: The team can show where the adjudication diverged from expectation and whether that divergence reflects a pattern.
Those are audit outputs. They also happen to be the exact building blocks you need when a claim moves into appeal or dispute.
Why this matters for underpayment strategy
Many organizations still run audits as if overpayment risk is the only issue. That leaves money on the table. In several specialty and facility-based settings, underpayment deserves equal attention. A claim can be technically clean and still be paid incorrectly.
When teams review remittances against audit findings, they start to see recurring payer behavior. Certain code families may be discounted more aggressively. Certain modifiers may trigger adverse adjudication. Certain service combinations may be consistently repriced or challenged. Without an audit framework, those patterns remain anecdotal. With one, they become actionable.
The operating model that works
The strongest model links three functions that are too often separated:
| Function | What it contributes |
|---|---|
| Medical billing audits | Detects error classes, documentation gaps, coding drift, and payment variance |
| Revenue cycle management | Supplies workflow data, claim outcomes, remittances, and operational ownership |
| IDR or appeal strategy | Converts clean documentation and pattern evidence into stronger dispute files |
That linkage is what turns audits from defensive compliance activity into financial infrastructure. It helps teams prevent weak claims upstream and prosecute underpayments downstream.
A claim is easiest to defend when the evidence was built before the dispute started.
Practices that understand this stop viewing audits as a burden imposed by payers or regulators. They use them to harden claims, improve recovery posture, and create a cleaner record when payment disputes reach formal escalation.
RevGuard helps specialty practices, facilities, and multi-state provider groups connect audit intelligence to real reimbursement outcomes. If your team needs cleaner claims, tighter revenue cycle controls, and stronger payer dispute execution under the No Surprises Act, RevGuard is built for that work.