
An 18% decline in professional reimbursement for gastroenterology services between 2018 and 2022, alongside an 11% drop in procedure frequency and a 7% drop in participating gastroenterologists, changes how a practice has to think about billing. This isn't just a collections issue. It is a margin protection issue tied directly to service capacity and long-term viability, as reported in this PubMed analysis of gastroenterology reimbursement trends.
In this environment, gastroenterology billing can't sit in the back office as a clerical function. It has to operate like a control system. Coding has to reflect what occurred. Documentation has to prove medical necessity without gaps. Denial management has to identify repeat payer behavior, not just resubmit claims. And when underpayments persist, the practice needs a dispute path that starts with a clean claim and ends with enforceable escalation.
The Financial Realities of Modern Gastroenterology
Shrinking reimbursement changes the math
An 18% reimbursement drop changes more than payer mix assumptions. It changes the tolerance for billing error.
In gastroenterology, a missed modifier, weak procedure note, or avoidable bundling mistake can erase margin on a case that was already paid below historical levels. The loss does not stop at one claim. It shows up in staffing decisions, physician compensation pressure, slower technology investment, and less room to absorb payer delays or audit activity. As noted earlier, reimbursement and procedure volume have both moved in the wrong direction. Relying on volume to offset preventable write-offs is a weaker strategy than it was a few years ago.
Many groups default to tactical fixes under that kind of pressure. They ask staff to work aged A/R harder, replace a biller, or appeal denials one by one without tracing the pattern back to scheduling, coding, documentation, or charge review. That can produce a temporary lift, but it rarely fixes the revenue leak.
Practical rule: Protect revenue before claim submission. A clean claim with the right coding logic costs less to produce than a corrected claim, an appeal, or a preventable write-off.
Billing now determines operational resilience
A stable GI revenue cycle is not just a collections function. It is a control system for yield.
That is especially true in gastroenterology, where payment often turns on small but decisive details. A colonoscopy may start as screening, convert to diagnostic or therapeutic work, and trigger a different payment path based on findings, symptoms, payer rules, and patient cost-sharing. If the documentation, diagnosis linkage, and modifiers do not match that sequence, the practice can lose revenue, create patient balance problems, or both.
The highest-performing teams do three things consistently:
- Protect yield at charge entry: Claims go out with the correct CPT code, diagnosis linkage, modifiers, and payer-specific edits already applied.
- Support medical necessity in the note: Documentation shows indication, findings, technique, interventions, and any change from screening to diagnostic or therapeutic service.
- Treat underpayments as contract issues, not posting issues: Staff compare payer payment to expected allowed amounts and pursue variances instead of accepting short pay as routine.
This is also where billing connects directly to dispute strategy. If a practice cannot prove what was done and why it was medically necessary, it has little footing when contesting a denial, an underpayment, or an out-of-network payment dispute under the No Surprises Act. Clean coding and defensible documentation are the front end of revenue recovery, not a separate project.
For practices tightening this process, a specialty-focused medical coding resource for healthcare claims can help standardize internal review and reduce variation across common GI encounters.
The groups that hold margin are usually not the ones chasing every denial the hardest. They are the ones that remove repeat errors, close the screening-versus-diagnostic gap, and build a billing operation that supports recovery from the first claim through final payer dispute.
Core Coding for Common GI Procedures
Start with a usable coding map
Most coding problems in gastroenterology billing don't begin with exotic cases. They begin with common procedures billed inconsistently. Staff know the broad code family, but they miss the detail that changes payment. That usually happens when charge entry relies on memory, old cheat sheets, or generic billing support.
A better approach is a short internal reference tied to your physicians' actual case mix. The table below is not a replacement for current payer policy, CPT guidance, or coder review. It is a working map for audit and training.
Common Gastroenterology CPT and Example ICD-10 Codes
| Procedure | CPT Code | Common ICD-10 Codes (Examples) |
|---|---|---|
| Colonoscopy, diagnostic | 45378 | Z12.11, K62.5, R19.4 |
| Colonoscopy with biopsy | 45380 | K63.5, K62.5 |
| Colonoscopy with snare removal | 45385 | K63.5 |
| EGD, diagnostic | 43235 | R10.13, K21.9 |
| EGD with biopsy | 43239 | K29.70, K21.9 |
| ERCP | 43260 | K83.1, K80.50 |
These are common examples, not a universal billing template. The code that gets paid is the one supported by the documented indication, findings, and intervention. If the physician performs a diagnostic exam and then adds therapy, the procedural code has to follow the highest supported service performed.
For teams reviewing their internal workflows, a specialty-focused medical coding resource for healthcare claims is useful when building cross-checks between physician documentation, charge capture, and claim edits.
Where practices usually go wrong
The pattern is familiar:
- They code from the schedule, not the op note. A screening label entered pre-procedure survives the encounter even after findings change the billing path.
- They use broad diagnoses when specificity exists. That weakens medical necessity support and creates avoidable payer review.
- They don't reconcile pathology, findings, and final CPT selection. The procedure note says one thing. The claim says another.
A GI coding workflow should force a final review after the procedure, not before it. The scheduler can capture intent. The biller has to capture reality.
The most expensive coding mistake is often the one your staff thinks is routine.
A practical audit lens
If you want to test whether your baseline coding is stable, pull a sample of recent EGDs, colonoscopies, and ERCPs and compare four fields only:
- Scheduled indication
- Final procedure note
- Submitted CPT and ICD-10 pair
- Paid amount and denial remarks
That comparison shows whether the problem is front-end classification, physician note quality, coder interpretation, or payer processing. In GI, those are different problems and they need different fixes.
The Documentation Mandate That Prevents Denials
Documentation is the claim's evidence file
In gastroenterology billing, documentation isn't an administrative burden. It is the proof packet that justifies payment. If the note is thin, the claim is weak even when the code itself looks correct.
That's why this matters so much: failure to submit accurate and specific documentation is the single leading cause of claim denials in gastroenterology, particularly when procedure notes lack details on technique or findings and payers deny for non-medical necessity, as outlined in this gastroenterology billing guide focused on documentation and denials.
Practices often try to solve denials downstream with appeals language. That helps only when the chart already contains what the payer needed. If the note never states the anatomical findings, method used, extent reached, specimen handling, or reason for intervention, the appeal is weak from the start.
What must appear in the record
A denial-resistant GI note usually answers a short set of practical questions:
- Why was the procedure performed? The indication has to match the diagnosis path and support medical necessity.
- What exactly was done? Diagnostic exam, biopsy, removal, control of bleeding, dilation, or another intervention.
- What technique was used? The record should distinguish methods when they affect coding or payer review.
- What did the physician find? Site, size, character, and number of lesions or abnormalities when applicable.
- What was collected or sent? Specimens, pathology handling, and labeling should be clear.
- Were there complications or deviations? If the case changed course, the note should explain why.
The goal isn't longer notes. The goal is notes that answer payer questions before they get asked.
How to tighten physician documentation without creating friction
The fix isn't to tell physicians to "document better." That fails because it is too vague. Good practice managers build structure around the note.
Use tools and habits like these:
- Procedure-specific templates: EGD, colonoscopy, ERCP, and therapeutic variants should not share the same generic note shell.
- Required fields for billing-sensitive items: Force completion for extent, findings, intervention type, and specimen details before sign-off.
- Coder feedback loops: When coders have to query the same physician for the same omission, turn that into a template revision, not a recurring email chain.
A strong appeal starts in the procedure room. If the note is incomplete on day one, revenue recovery gets harder with every handoff.
Compliance matters here too
Imprecise documentation doesn't just slow payment. It also creates exposure. Overcoding, vague language, and unsupported medical necessity can trigger payer scrutiny and federal audit risk. That's one reason the most stable GI practices treat documentation review as both a revenue function and a compliance function.
The cleanest operations make physicians' documentation easier to complete and easier to validate. That is what keeps claims moving and keeps auditors from finding preventable gaps.
Mastering Modifiers and Navigating Payer Rules
Modifiers separate valid reimbursement from avoidable leakage
Modifiers are where many GI claims stop being straightforward. The code may be right, the diagnosis may be justified, and the claim can still underpay if the modifier logic is wrong or missing. This is especially common in endoscopy families, where multiple services, edits, and preventive benefit rules interact.
Here is the visual checklist I use when training staff to slow down before submission:
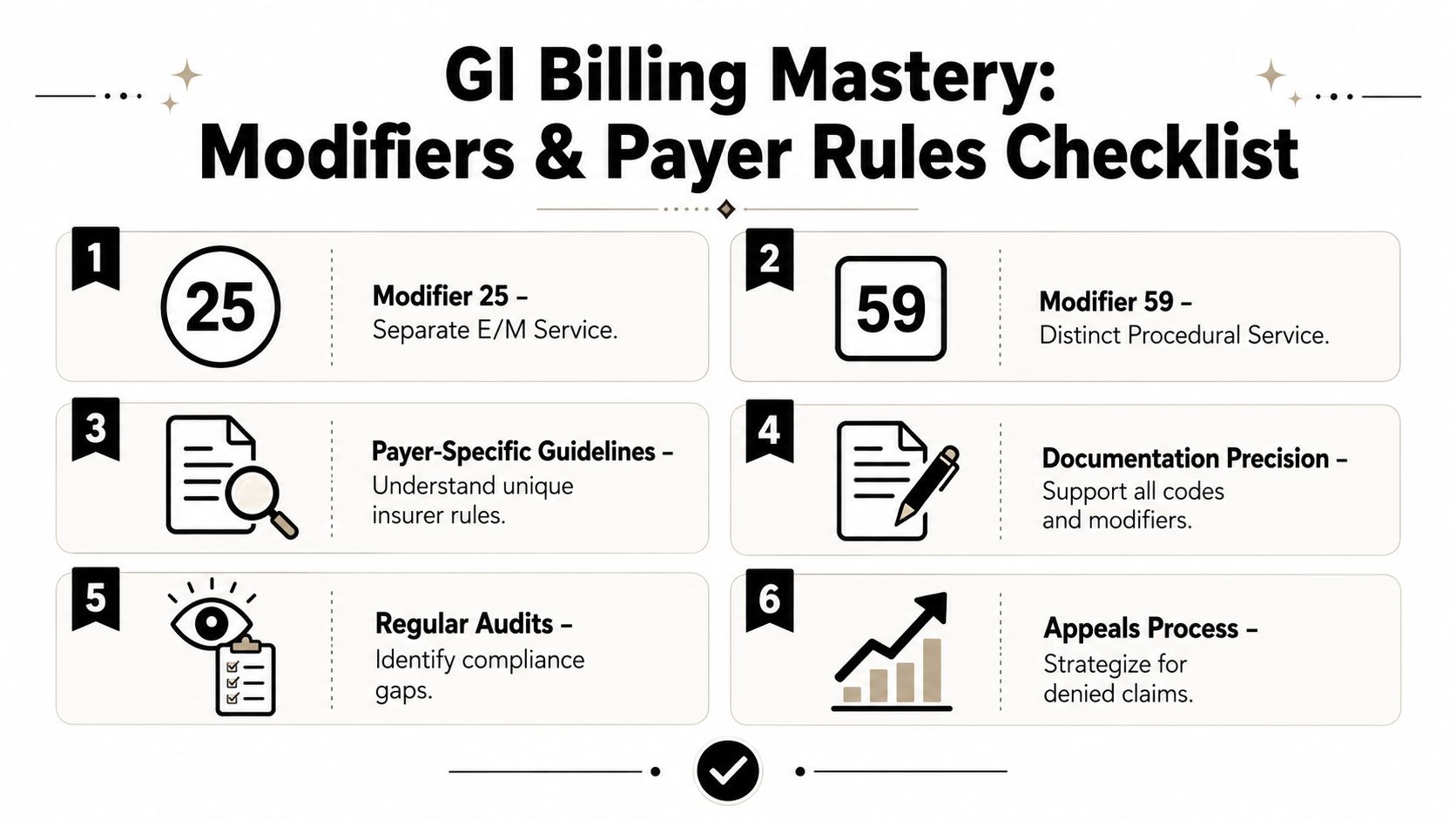
A generic billing team usually knows modifiers exist. A good GI billing team knows when a modifier is the difference between proper reimbursement and a silent write-off.
The screening versus diagnostic trap
This is one of the most consequential workflow failures in gastroenterology billing. The issue isn't only that staff pick the wrong code. The issue is that the billing workflow doesn't update when the clinical reality changes during the procedure.
The systemic failure to update a screening colonoscopy code to a diagnostic one after a polyp is found is a primary reason GI practices lose an estimated $140,000 to $220,000 annually, according to this analysis of hidden GI revenue loss tied to screening-to-diagnostic conversion.
That number gets attention, but the operational lesson matters more. The error usually begins upstream:
- The case is scheduled as preventive.
- Staff build the claim path around that preventive status.
- The physician finds a lesion or removes a polyp.
- The final billing logic doesn't fully reconcile the procedure note, diagnosis sequence, and modifier requirements.
This is not a coder typo. It is a broken handoff between scheduling, the procedure room, charge capture, and final billing review.
What reliable modifier logic looks like
A useful internal rule is simple. Never let the scheduled intent control the final claim without post-procedure reconciliation.
For GI teams, that means checking:
- Modifier 25 when a separate E/M service is properly supported on the same date.
- Modifier 59 when a distinct procedural service is separately reportable and documentation supports that distinction.
- Modifier 51 when multiple procedures require sequencing review under payer rules.
- Modifier PT or preventive modifiers where applicable when a screening service converts based on findings and the payer requires a specific indicator.
Not every payer processes these the same way. That is exactly why payer policy matrices matter. One carrier may honor a claim with standard edit logic. Another may require plan-specific sequencing or diagnosis placement to preserve payment.
If your staff has to guess whether a modifier applies, the workflow is already too loose.
Build the workflow around the final operative reality
The strongest GI teams use a post-procedure checkpoint before claim submission. It doesn't need to be complicated. It does need to be disciplined.
A practical review queue should answer:
| Review point | What staff should confirm |
|---|---|
| Scheduled indication | Was the case booked as screening, surveillance, or symptom-based? |
| Final finding | Did the physician identify a polyp, lesion, bleeding source, stricture, or another abnormality? |
| Intervention performed | Was tissue sampled, removed, cauterized, dilated, or otherwise treated? |
| Modifier need | Do payer edits require modifier logic to preserve separate reimbursement or preventive status indicators? |
| Diagnosis order | Does the final diagnosis sequencing reflect the encounter as performed, not as scheduled? |
When this review is skipped, the claim often still gets submitted. It just gets paid incorrectly, denied, or shifted to patient responsibility in ways that trigger avoidable callbacks and rework.
A Proactive Framework for Denial Management
Denials should be categorized, not chased
Most practices handle denials as incoming noise. Staff work whatever appears in the work queue, fix the immediate issue, and move on. That approach keeps the queue moving, but it doesn't reduce future denials.
In gastroenterology, that is expensive. Between 23% and 31% of gastroenterology practices using generalist billing companies experience systematic endoscopy bundling errors, according to MGMA benchmark data discussed in this review of GI billing company performance. That matters because bundling problems are usually repeatable. If one claim is wrong, many claims are wrong.
This infographic captures the mindset shift well:
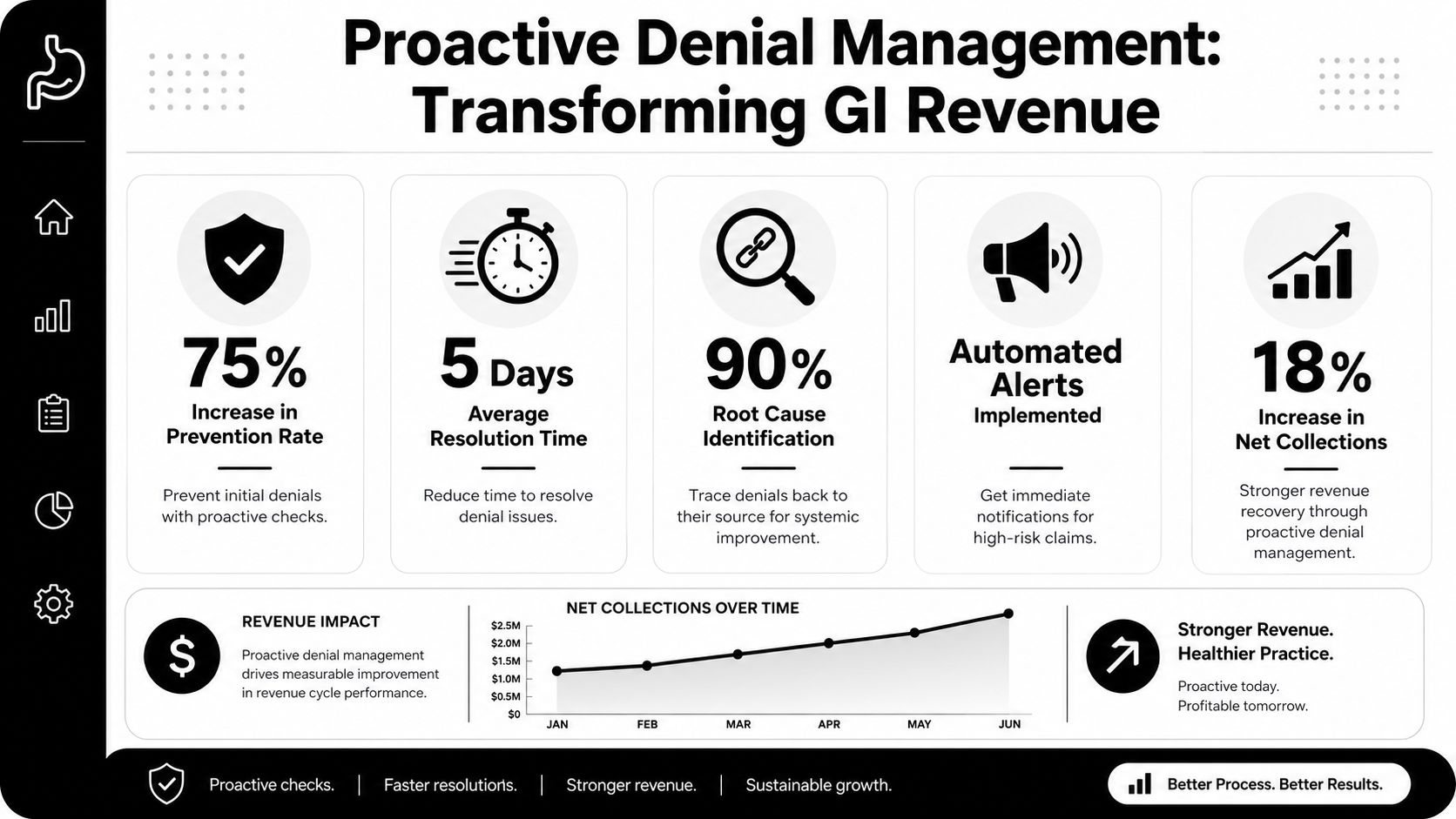
A GI denial program should identify patterns by type, payer, location, and physician. If your team only knows the denial code, but not the root cause category, it can't fix the system.
A working denial framework
Use categories that map to action. For most GI practices, these are enough:
- Front-end denials: Eligibility, registration mismatch, prior authorization, coordination of benefits.
- Clinical support denials: Medical necessity, missing records, insufficient documentation.
- Coding and edit denials: Modifier errors, bundling, diagnosis mismatch, duplicate logic.
- Payment variances: Underpayments, downcoding, contract misapplication, carve-out disputes.
A structured healthcare denial management approach for specialty practices helps when you want to turn these categories into recurring worklists, ownership rules, and payer-specific edits.
Close the loop with operations
A denial team that only resubmits claims stays busy forever. A denial team that reports root causes changes practice performance.
Use monthly review to ask questions like:
- Which denial category rose this month?
- Did one payer introduce a new edit pattern?
- Are the same physicians missing the same documentation elements?
- Did a registration script change create front-end fallout?
Then assign fixes where they belong. Registration should own eligibility errors. Coding should own edit logic. Physicians should get concise feedback only on chart deficiencies they can change.
The point of denial management isn't faster rework. It's fewer denials entering the system in the first place.
Advanced Revenue Recovery and Dispute Resolution
Clean claims are only the first layer
Even a well-run GI billing operation will still encounter underpayments, delayed payments, and payer interpretations that don't match the contract or the clinical record. That is where many practices stop too early. They appeal once, get a partial response, then post the balance off as a difficult account.
That leaves money on the table and teaches the payer a bad lesson. If the payer learns your group won't escalate, payment behavior usually doesn't improve.
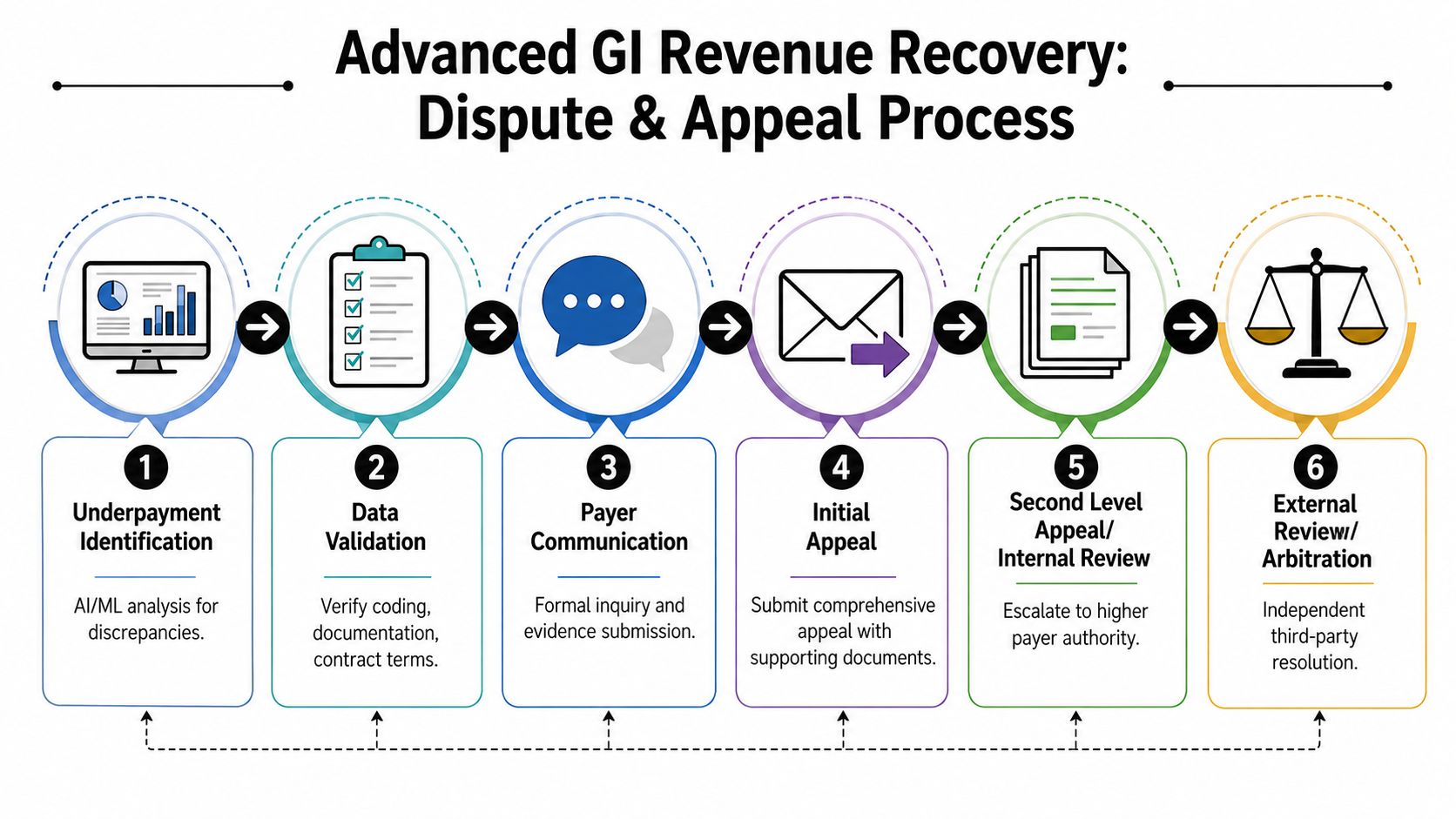
This is the escalation path teams need to understand:
Build dispute-ready claims from day one
A recoverable underpayment starts with a claim file that can survive scrutiny. That means the practice should be able to assemble, quickly and consistently:
- The operative documentation
- Diagnosis and procedure rationale
- Modifier support
- Payer policy references when relevant
- Contract terms or reimbursement methodology
- A payment variance summary showing what was expected and what was received
When those elements are scattered across the EHR, PM system, shared drives, and staff email, escalation becomes too slow and too inconsistent. That's why the strongest revenue recovery models tie claim production and appeals evidence together from the beginning.
Where the No Surprises Act changes strategy
For eligible out-of-network payment disputes, the No Surprises Act and the Independent Dispute Resolution process create a formal path beyond routine payer appeals. In practical terms, this means some underpayments are no longer just billing disagreements. They can become structured disputes with defined evidence requirements and a third-party review process.
That shifts how a practice should think about difficult claims. Instead of asking, "Can we get the payer to reconsider?" the better question is, "Did we create a record strong enough to support formal dispute escalation if internal review fails?"
Enforcement matters. A practice can submit technically clean claims and still lose revenue if it has no process for identifying underpayments worth escalating, packaging evidence, and meeting dispute deadlines.
An effective recovery ladder
A workable escalation ladder in GI looks like this:
Variance identification
Payment posting flags claims that don't match expected reimbursement logic.Internal validation
Staff confirm coding, documentation, modifier use, and payer responsibility before escalating.Targeted payer challenge
The appeal addresses the exact reason for underpayment, not a generic request for review.Second-level escalation
If the payer response is incomplete or unsupported, the dispute advances with a tighter evidence packet.External dispute path when applicable
For qualifying claims, the practice evaluates whether formal arbitration or related review mechanisms should be used.
One option in this space is RevGuard, which combines specialty-specific RCM workflows with IDR support under the No Surprises Act, linking claim preparation, underpayment analysis, evidence assembly, and escalation in a single process. The key point is not the vendor name. The key point is that your billing operation needs a real bridge between front-end claim accuracy and back-end enforcement.
What doesn't work
Three habits consistently weaken advanced revenue recovery:
- Generic appeals language: Payers ignore broad complaints that don't isolate the variance.
- Late evidence gathering: If staff start hunting for records after the denial window narrows, their effectiveness is reduced.
- No threshold rules: Teams need criteria for which underpayments justify appeal, escalation, or formal dispute activity.
Practices that recover the most revenue aren't always the ones with the biggest billing teams. They are usually the ones with tighter issue triage, better supporting records, and a clear escalation protocol.
Building a High-Performance GI Revenue Cycle
Revenue protection starts before the procedure
A small number of workflow failures drive a large share of GI revenue loss. In practice, the same problems keep showing up: eligibility errors, missed screening-to-diagnostic changes, weak claim edits, underpayment write-offs, and patient statements that create confusion instead of payment.
A high-performance gastroenterology billing operation treats the revenue cycle as one connected system. The handoff from scheduling to registration affects coding. Coding affects payer response. Payer response affects patient balances. If those teams work in silos, cash slows down and preventable write-offs rise.
This kind of dashboard view helps leadership spot where performance is slipping:
For groups building tighter controls across the full claim lifecycle, gastroenterology revenue cycle support for GI practices shows how eligibility, coding edits, denial prevention, underpayment review, and patient collections can be aligned in one workflow.
The operating model that holds up
GI practices get better financial results when each stage has a clear owner and a defined financial checkpoint.
Before the visit or procedure
Confirm active coverage, site-of-service rules, prior authorization requirements, and the patient's likely cost share. Flag screening colonoscopies that may convert to diagnostic or therapeutic based on findings, because that is one of the fastest ways to create downstream billing disputes.After the procedure
Match the procedure note, pathology, and charge entry before the claim drops. In GI, small documentation gaps around polyp removal, biopsies, or indication sequencing can change payment and patient liability.At claim release
Apply payer-specific edits for NCCI bundling, modifier support, diagnosis order, frequency limits, and place-of-service requirements. Clean claim rate matters, but so does whether the claim can survive an audit or appeal later.After adjudication
Compare the remittance to expected reimbursement, not just the amount paid. A posted payment is not proof of correct payment. It may be a short pay that needs contract review, appeal, or formal dispute evaluation.At patient balance stage
Send a statement the patient can understand and the staff can defend on the phone. If the balance changed because a preventive service became diagnostic, the statement and call script should explain that clearly.
Patient billing clarity affects collections
Many GI groups spend heavily on coding and still lose cash after adjudication because the patient-facing bill is vague. That problem shows up in slower self-pay collections, more inbound calls, and more balances that age out.
The fix is plain language. Patients need to see what was done, what insurance processed, why a balance remains, and what changed if a screening service became diagnostic. Confusing terminology creates hesitation, and hesitation delays payment, as noted in this analysis of patient billing communications.
Clear patient billing language is a collections tool.
Track fewer metrics, but use metrics tied to action
A GI practice does not need a sprawling KPI report. It needs a short scorecard tied to revenue risk, root cause, and accountability.
| KPI area | What it tells you |
|---|---|
| Clean claim performance | Whether front-end controls and coding edits are preventing rework before submission |
| Screening vs. diagnostic variance | Whether colonoscopy coding, patient estimates, and final liability are staying aligned |
| Denial categories by payer | Which payer rules or internal failures are creating repeat losses |
| Underpayment variance | Whether paid amounts match contract expectations and whether escalation rules are being followed |
| Days in A/R by financial class | Where cash is slowing across payer and patient balances |
| Patient collection response | Whether statement clarity, call handling, and payment options are converting balances into cash |
The strongest GI revenue cycles are built for prevention and recovery. They catch errors before claim submission, identify underpayments after posting, and support escalation when payer behavior requires more than a standard appeal. That includes knowing when a disputed out-of-network payment may justify action under the No Surprises Act IDR process instead of another round of routine follow-up.
If your gastroenterology practice needs tighter coordination between specialty billing operations and recovery of delayed, denied, or underpaid claims, RevGuard provides GI-focused RCM and IDR support built for that workflow. The practical goal is straightforward: cleaner claims on the front end, stronger evidence on the back end, and fewer revenue leaks across the entire cycle.