
If you own or lead a practice right now, you're probably balancing two jobs that don't fit neatly together. One is medicine. The other is protecting cash flow while staffing stays tight, payer behavior stays unpredictable, and administrative work keeps spreading into every part of the day.
That's why medical practice management can't be treated as front-desk coordination plus billing follow-up. In a healthy practice, it functions as the financial operating system. It shapes how quickly you get paid, how much revenue slips away before anyone notices, and whether your team is solving the right problems or constantly reacting to avoidable ones.
Why Medical Practice Management Is Now Mission-Critical
A lot of physician-owners still think of management as overhead. That view is outdated.
Medical practice management now sits at the center of practice viability because the business side of medicine has become more demanding, not less. Payer edits are tougher. Documentation expectations are tighter. Staffing gaps expose weak workflows fast. A practice can be clinically strong and still struggle financially because its management model doesn't protect reimbursement.
The stakes are bigger than most practices realize
The scale of the industry tells the story. The U.S. medical group practice management sector is projected to reach $210.4 billion in 2026, and it expanded at a 9.5% compound annual growth rate from 2020 to 2025, according to IBISWorld's medical group practice management industry outlook.
That growth matters for one reason. More money, more consolidation, and more operational complexity create a tougher environment for independent groups, specialty practices, ASCs, and multi-site platforms. The practices that treat management as strategy will usually outperform the ones that treat it as paperwork.
A strong management model does four things at once:
- Protects revenue: It catches eligibility issues, coding gaps, and payer friction before they turn into write-offs.
- Stabilizes operations: It gives staff clear workflows instead of constant exceptions.
- Supports growth: It makes expansion possible without multiplying chaos.
- Creates visibility: It lets leadership see whether the problem is volume, collections, denials, staffing, or contract performance.
Practical rule: If you can't explain where cash is getting delayed or lost, your practice doesn't have a billing problem alone. It has a management problem.
Survival now depends on financial discipline
The most successful practices don't separate operations from reimbursement. They connect scheduling, eligibility, documentation, coding, claims, follow-up, and dispute escalation into one managed system.
That's also why many groups are rethinking how they approach revenue cycle optimization for specialty practices. The point isn't to bill faster. It's to build a structure where clean claims go out the first time, underpayments are visible, and leadership can act before leakage becomes normal.
Medical practice management used to sound administrative. Today, it's a strategic financial function. Practices that accept that shift tend to make better decisions about staffing, software, payer strategy, and growth.
The Seven Pillars of a Modern Medical Practice
A modern practice works like a building. If one support column weakens, pressure shifts to the others. Billing starts compensating for scheduling mistakes. Physicians start compensating for staffing gaps. Managers start compensating for poor systems. That's when people get burned out and revenue gets messy.
The better approach is to treat medical practice management as seven connected pillars.
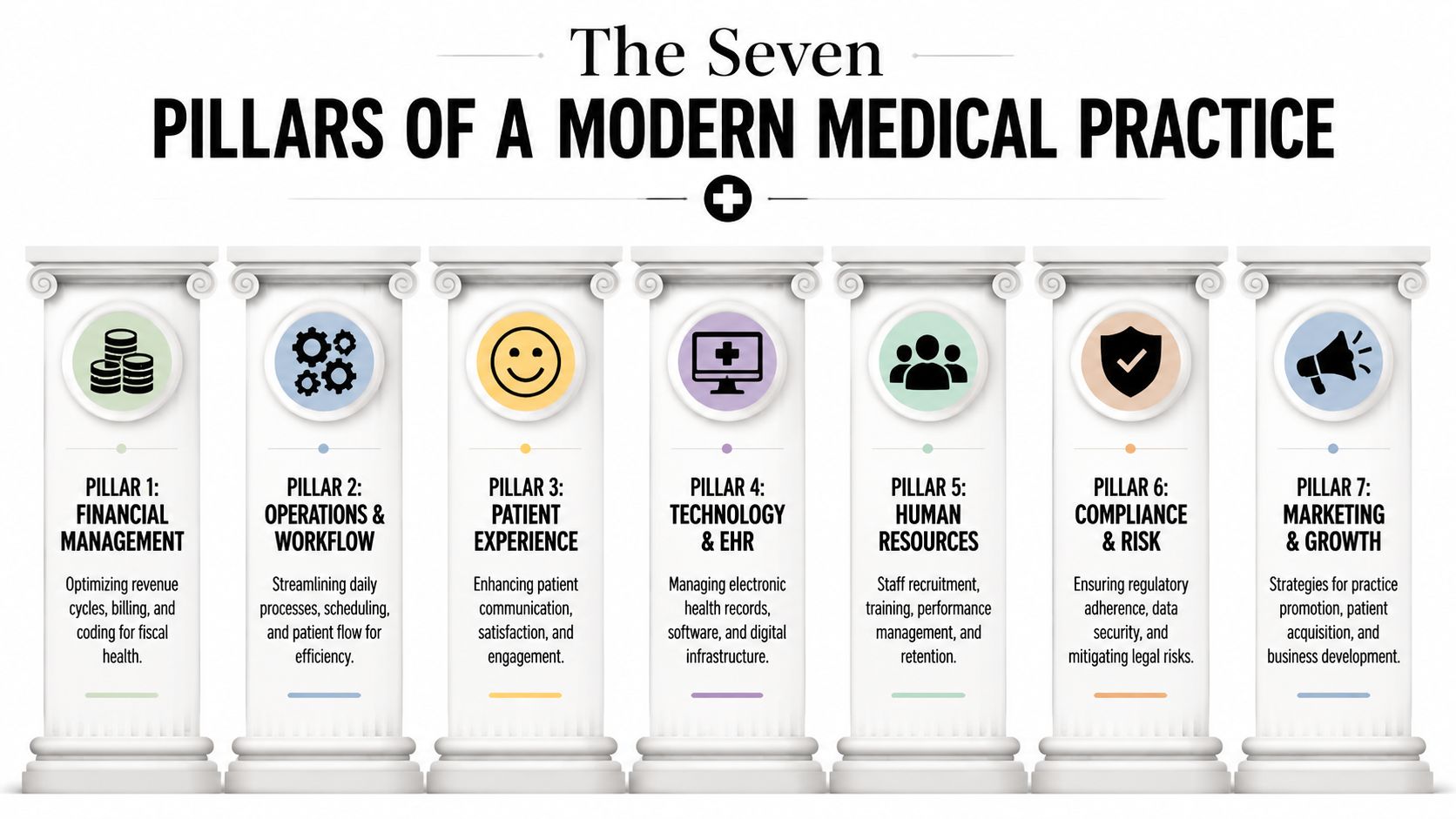
Financial management
This pillar decides whether the practice converts work into cash. It includes charge capture, coding oversight, claim submission, payment posting, denial follow-up, and patient balance workflows.
If this area is weak, everything downstream gets harder. The practice may stay busy while cash lags behind production, which is one of the most common reasons leaders feel confused by their own numbers.
Operations and workflow
Operations determine whether the office runs on repeatable processes or daily improvisation. Scheduling templates, intake, prior authorization handoffs, referral coordination, and checkout all live here.
Good workflow design reduces rework. Bad workflow design pushes avoidable problems into billing, where they become denials.
Patient experience
Patient experience isn't separate from practice economics. It affects registration quality, collections conversations, appointment adherence, portal use, and trust.
A patient who understands financial responsibility and receives clear communication is easier to collect from than a patient who feels surprised, confused, or ignored.
Most practices don't lose money in one dramatic event. They lose it in small operational misses that repeat all week.
Technology and EHR
Software should reduce friction, not create it. Your practice management system and EHR should help staff move information cleanly across scheduling, clinical documentation, and billing.
A robust PMS should include AES-256 encryption, granular access controls, and immutable audit logs. It should also support EHR interoperability, and the vendor should provide a signed Business Associate Agreement for HIPAA and No Surprises Act compliance. Those aren't technical extras. They're operational requirements.
When a group reviews its stack, the issue usually isn't whether it owns software. It's whether the tools support the actual work. Credentialing workflows, for example, often sit in a separate process that delays payer readiness if nobody owns it tightly. That's why many groups formalize provider credentialing workflows and enrollment oversight instead of leaving them fragmented across departments.
Human resources
Hiring is only one part of this pillar. Training, accountability, role clarity, and retention matter just as much.
A strong front desk with weak training can create financial damage quickly. The same is true for billers who are overloaded, supervisors who don't audit work, or managers who tolerate process drift because everyone is already busy.
Compliance and risk
Compliance isn't just about passing audits. It affects how safely your practice handles patient information, payer documentation, refunds, dispute files, and legal exposure.
The practices that handle compliance well don't treat it as a binder on a shelf. They build it into workflows, permissions, documentation habits, and vendor oversight.
Marketing and growth
Growth should be profitable, not just visible. New locations, new providers, and new referral relationships only help if the practice can operationalize them without weakening collections or patient access.
A practical way to view the seven pillars is this:
| Pillar | What it protects |
|---|---|
| Financial management | Cash flow and reimbursement |
| Operations and workflow | Efficiency and consistency |
| Patient experience | Retention and collections trust |
| Technology and EHR | Accuracy and visibility |
| Human resources | Execution and stability |
| Compliance and risk | Legal and contractual protection |
| Marketing and growth | Sustainable expansion |
When these pillars work together, management stops feeling reactive. It starts acting like infrastructure.
Measuring Success and Spotting Trouble
Most practice leaders can sense when something's off. Cash is slower. Staff sound more frustrated. Claims feel stuck longer than they should. The problem is that intuition alone doesn't tell you where the breakdown sits.
A manageable KPI set does.
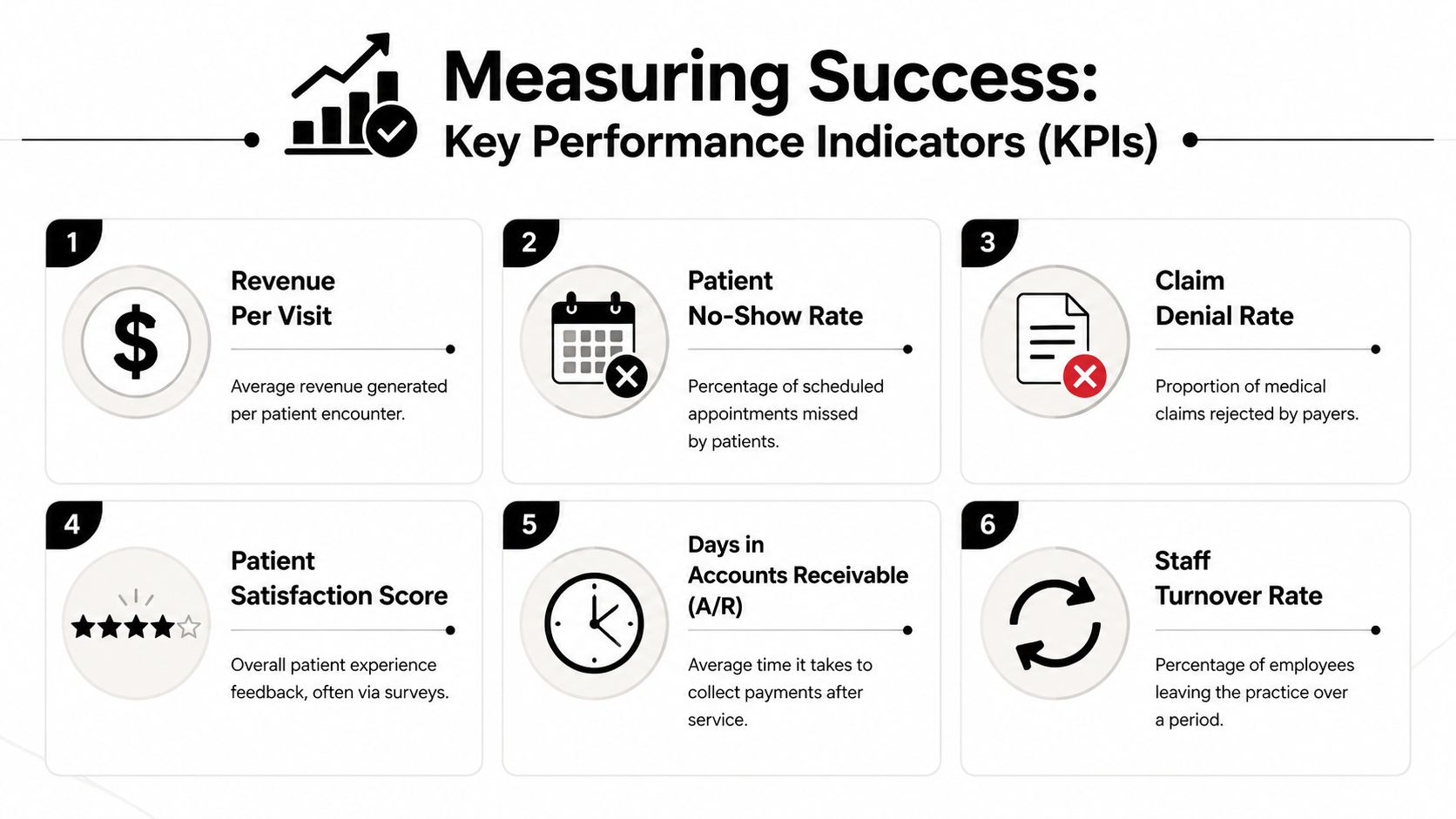
The three numbers that deserve executive attention
According to the MGMA KPI white paper on practice revenue cycle performance, an optimal claim denial rate should stay below 5%, Days in A/R should be 30 to 40 days, and Net Collection Rate should be 95% to 97%.
Those aren't abstract finance targets. They tell you whether the practice is collecting what it should, how long cash is trapped in the cycle, and whether avoidable friction is spreading.
Here's how to read them in plain business terms:
- Claim denial rate below 5%: You're preventing a large share of avoidable payer rejection.
- Days in A/R at 30 to 40 days: Cash is moving at a pace that supports payroll, vendors, and reinvestment.
- Net Collection Rate at 95% to 97%: The practice is converting collectible revenue into actual payment with limited leakage.
What trouble looks like in real operations
When denial rate rises, the symptom isn't only more denied claims. Staff spend more time reworking claims, physicians get more documentation questions, and managers lose visibility because everyone is chasing exceptions.
When Days in A/R drifts upward, the pressure lands on leadership decisions. You start delaying hires, questioning growth plans, or tightening expenses because cash timing no longer matches production.
When Net Collection Rate falls, the practice usually has one of three issues. It may be undercoding, missing follow-up discipline, or accepting payer behavior that should be challenged.
A healthy practice doesn't just produce revenue. It collects predictable cash from that production.
A short diagnostic checklist
Review these questions with your billing lead or administrator:
- Are denials categorized clearly: If your team can't separate eligibility, authorization, coding, and payer-edit denials, root causes stay hidden.
- Is aging actively worked: Old A/R doesn't improve because someone runs a report. It improves because staff own deadlines and escalation paths.
- Are underpayments visible: Many practices post payments and move on. That habit hides payer behavior.
- Do physicians see KPI trends: Provider leaders don't need every report, but they do need a dashboard that links operations to reimbursement.
One caution matters here. Don't overload your practice with vanity metrics. Revenue per visit, no-shows, staffing turnover, and patient satisfaction all matter, but the three KPI benchmarks above tend to expose the core financial condition fastest. If those numbers are weak, there's usually a structural issue somewhere in intake, coding, billing workflow, or payer follow-up.
In-House vs Outsourced Practice Management
This decision is rarely philosophical. It's operational.
Some groups want full internal control because leadership is used to walking down the hall to solve problems. Others outsource because they're tired of rebuilding billing teams, training around turnover, or trying to create payer expertise across multiple specialties. Both models can work. Both can fail.
The right question is simpler. Which model gives your practice reliable execution, financial visibility, and enough expertise for your payer mix?
Where in-house teams usually perform well
In-house teams often do best when the practice is stable, leadership is hands-on, and the workflows are relatively consistent. There's immediate access to staff. Physicians can escalate issues directly. Culture alignment tends to be stronger when teams work shoulder to shoulder.
But internal teams also create concentration risk. If key billing or management staff leave, knowledge leaves with them. Training becomes continuous. Specialty-specific payer strategy can be hard to build if the practice doesn't have enough scale to support deep expertise.
Where outsourced models usually add value
Outsourced partners can bring process discipline, broader payer exposure, and mature reporting that would take time to build internally. That matters most when the practice is multi-site, growing quickly, or dealing with recurring denial and underpayment patterns that basic billing follow-up isn't fixing.
The strongest advantage appears when outsourced support integrates routine revenue cycle work with downstream dispute escalation. Data from the AMGA shows that 86% of practices with integrated RCM/IDR workflows reported a 25% reduction in net denials within 12 months, while practices managing those functions separately saw a 15% increase in revenue leakage.
That doesn't mean outsourcing is automatically better. It means separation between front-end billing and downstream enforcement creates a weakness. Some outsourced firms close that gap better than internal teams can.
Here's a practical side-by-side view:
| Factor | In-House Team | Outsourced Partner |
|---|---|---|
| Control | Direct day-to-day oversight | Less direct, depends on governance |
| Staffing risk | Recruiting and turnover sit with the practice | Partner absorbs more execution risk |
| Specialty expertise | Varies by who you can hire | Often broader if partner focuses on healthcare reimbursement |
| Scalability | Harder during growth or multi-site expansion | Easier to expand if workflows are standardized |
| Technology and analytics | Built internally or pieced together | Often included as part of service model |
| Payer escalation | May be limited to standard appeals | Can be stronger if partner handles enforcement workflows |
| Cost structure | Payroll and management overhead are fixed | Service cost is external, but may reduce hidden inefficiency |
The trade-off most owners underestimate
The actual issue isn't cost on paper. It's management bandwidth.
If physician-owners or administrators spend too much time supervising workflow gaps, replacing staff, checking claim status problems, or sorting through denial noise, the internal model may look cheaper than it is. Time spent stabilizing weak execution is still a cost.
Some practices solve this with a hybrid approach. They keep scheduling, patient-facing operations, and local supervision in-house, while outsourcing specialized reimbursement functions. Firms such as specialty-focused revenue cycle management outsourcing partners are often used in that narrower role when a practice wants deeper payer strategy without giving up operational control.
The best model is the one your practice can govern well. If you can't measure performance, enforce accountability, and adapt quickly, the model is wrong even if it looks familiar.
Why Your Specialty Changes Everything
Generic advice breaks down fast in specialty medicine.
A multispecialty article might tell you to improve coding accuracy, tighten front-end verification, and appeal denials quickly. That's all fine. It also misses the core issue. Each specialty has its own failure points, payer behaviors, and reimbursement pressure points. A workflow that works for dermatology may be useless in anesthesia, and a process built for routine office visits may collapse in air ambulance or hospital-based care.

Different specialties create different management burdens
Orthopedics often deals with procedural complexity, surgical scheduling coordination, imaging ties, and documentation that has to support medical necessity cleanly from referral through post-op billing.
Cardiology frequently runs into layered service lines, diagnostic documentation demands, and payer scrutiny around testing and procedural support.
Dermatology may look simpler from the outside, but high visit volume, mixed procedure types, cosmetic versus medical distinctions, and collection discipline can make margin protection highly dependent on clean front-end processes.
Anesthesia and emergency-related specialties face a different kind of pressure. They often have less control over patient acquisition and stronger exposure to payer underpayment behavior. In those settings, management can't stop at claim submission. It has to account for enforcement.
Air ambulance and other high-friction specialties need a different model
Air ambulance is the clearest example. This segment faces denial rates over 40%, yet general practice management guidance rarely includes a workable protocol for building the IDR engine needed to convert those underpayments into recoverable revenue under the No Surprises Act.
That gap matters because a specialty with unusual coding complexity, geography-related disputes, or frequent downcoding doesn't benefit much from generic billing advice. It needs workflows built around its actual reimbursement reality.
If your specialty attracts unusual payer scrutiny, standard denial management won't be enough. The practice has to be built for dispute readiness from the start.
What specialty-aware management looks like
A useful specialty model usually includes:
- Front-end rules built for that specialty: Eligibility, authorization, scheduling, and documentation prompts should reflect common denial triggers for the actual service line.
- Coding oversight that understands nuance: Not just coding in theory, but coding in the context of specialty documentation habits and payer edits.
- Payer pattern tracking: The team should know which plans downcode, stall, or underpay in repeatable ways.
- Escalation paths that match the risk: Some specialties can recover revenue through standard appeals. Others need formal dispute strategy.
That's why “best practices” in medical practice management should always be filtered through specialty economics. Otherwise the advice sounds polished but doesn't survive contact with your actual payer mix.
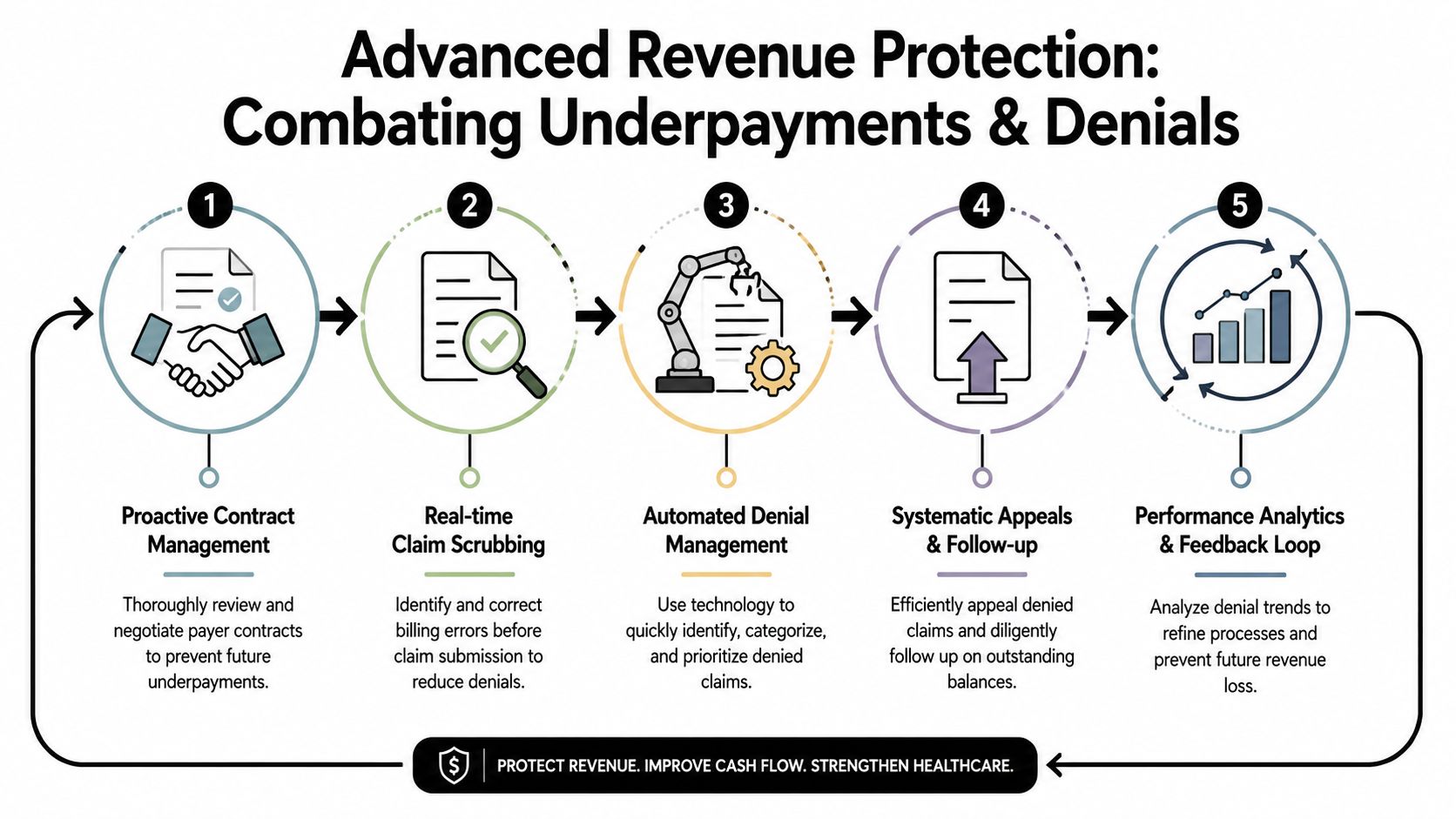
Beyond the Basics Advanced Revenue Protection
Traditional practice management assumes the revenue cycle ends when a claim is submitted cleanly and the billing team follows up on denials. That model no longer fits the payer environment many specialties face.
The more durable model treats revenue cycle management and Independent Dispute Resolution as one connected system. The goal isn't just fewer denials. It's stronger reimbursement defense from the first patient touch through final payment.
Clean claims are only the beginning
Most practices already understand the basics of clean claims. Verify coverage early. Code accurately. Submit fast. Track denials. Appeal what you can.
That work still matters. But it doesn't fully address a setting where some payers delay, underpay, or downcode in systematic ways. In that environment, a clean claim is necessary but not sufficient.
An advanced revenue protection model connects upstream actions with downstream enforcement:
- Eligibility and intake discipline to reduce preventable defects.
- Coding and claim construction that support the strongest payable position.
- Payer-response monitoring to identify patterns, not just single incidents.
- Structured appeals and evidence assembly when payment doesn't match the claim.
- IDR activation when appropriate under the No Surprises Act.
Why IDR belongs inside practice management
For certain specialties, dispute work isn't an occasional legal side process. It's part of reimbursement operations.
A critical gap still exists in how practices manage IDR. Air ambulance providers are a strong example because denial rates exceed 40% and generic guidance rarely provides a usable operating model for recovering those losses through NSA-compliant arbitration.
That's why I advise physician groups and specialty operators to stop treating IDR as a separate event handled after the business office has already failed. The stronger approach is to design the revenue cycle so claims are dispute-ready from the start. That means documentation, coding logic, audit trails, payer communications, and payment variance tracking all support possible escalation later.
Revenue protection starts before submission. By the time a payer underpays, the practice should already have the evidence structure it needs.
What changes in day-to-day operations
Once a practice adopts this mindset, a few operational habits change quickly:
- Teams track underpayments deliberately: Not just denials, but payments that don't match the expected value.
- Documentation supports enforceability: Staff collect and retain the records needed for appeals and arbitration.
- Analytics focus on payer behavior: Leadership watches patterns by payer, location, and service type.
- Escalation becomes policy-driven: Staff know when an issue stays in normal A/R and when it moves into dispute workflow.
This is the practical difference between routine billing and revenue protection. Routine billing tries to get paid. Revenue protection builds the practice to defend what it earned.
One firm operating in that model is RevGuard, which links specialty-specific RCM work with NSA-focused IDR workflows so claims can move from eligibility and coding through payer challenge and formal dispute enforcement within one operating structure.
Your Next Steps Toward a Resilient Practice
If your practice still treats management as scheduling, staffing, and billing oversight, you're probably carrying more financial risk than you think. The current environment rewards practices that run with discipline, visibility, and a plan for payer resistance.
That doesn't mean you need to overhaul everything at once. It means you need an honest read on where your current model is fragile.
A practical self-audit
Use this checklist at your next leadership meeting:
- KPI visibility: Do you review denial rate, Days in A/R, and Net Collection Rate consistently enough to spot deterioration early?
- Front-end reliability: Are eligibility, authorization, registration, and charge capture standardized, or do they depend on individual staff habits?
- Specialty fit: Does your management workflow reflect the actual denial and underpayment patterns of your specialty?
- Technology adequacy: Does your PMS support secure access, auditability, interoperability, and clean handoffs across the revenue cycle?
- Underpayment response: Can your team identify when a payer paid incorrectly, not just when it denied a claim?
- Escalation readiness: Do you have a clear path from billing issue to appeal to formal dispute action when needed?
The mindset shift that matters
A resilient practice doesn't wait for the monthly report to confirm a problem everyone already feels. It builds systems that surface risk early and respond with discipline.
That's the true shift in medical practice management. Stop thinking of it as administrative support for the clinical enterprise. Start treating it as the structure that protects reimbursement, stabilizes operations, and gives physician leadership room to make decisions from data instead of stress.
Practices that make that shift usually stop spending all their energy plugging leaks. They start building a business that can absorb pressure and still perform.
If your practice needs tighter control over denials, underpayments, and specialty-specific reimbursement workflow, RevGuard is one option to evaluate. It supports medical practice management through integrated revenue cycle operations and No Surprises Act dispute workflows, which can be useful for groups that need stronger revenue protection than standard billing support provides.