
You hire a strong clinician. Their schedule fills quickly. Staff starts routing patients, the physicians expect coverage relief, and finance expects revenue to follow. Then billing asks a simple question: is the provider fully credentialed and enrolled with every payer that matters?
If the answer is no, the provider credentialing process stops being an admin project and becomes a cash problem.
That's the mistake many practices make. They treat credentialing like paperwork that sits somewhere between HR, compliance, and medical staff services. In reality, it sits at the front of the revenue cycle. If the file is incomplete, if payer enrollment is inconsistent, or if recredentialing slips, claims don't just slow down. They deny, rework piles up, and cash gets trapped behind preventable operational errors.
Beyond Compliance Credentialing as a Revenue Function
A practice manager usually feels credentialing pain before anyone labels it correctly. Payroll has started. Clinic space is assigned. Schedules are live. But the new provider can't reliably bill in network yet, or can only bill some plans and not others. On paper, the hire is complete. In the revenue cycle, the hire is still unfinished.
That's why I don't treat the provider credentialing process as a compliance checklist. I treat it as revenue activation. The file you build at the start determines whether claims go out clean, whether payer records match your rendering and billing setup, and whether future denials are avoidable or baked in from day one.
Where financial leakage actually starts
Most operational teams think the problem is slow approval. Slow approval matters, but the larger problem is what bad setup does after approval. A sloppy file creates downstream defects that are harder to spot and more expensive to fix.
Common examples include:
- Mismatched provider data: The legal name, taxonomy, practice location, or group affiliation doesn't line up across payer records, billing setup, and claim submission.
- Partial enrollment: The provider is active with some plans but not others, so collections look inconsistent and no one catches the root cause quickly.
- Weak documentation control: A missing explanation for work history, inconsistent dates, or outdated documents trigger repeated follow-up and rework.
- Poor handoff to billing: Credentialing says approved, but billing doesn't know the effective date, linked tax ID, or participating status details.
Practical rule: If credentialing and billing teams don't share the same source of truth, denials will show up later as “payer issues” that actually started during onboarding.
The revenue impact is broader in organizations with layered payer mixes and distributed sites. Independent industry coverage notes that inefficient credentialing and mistakes increase costs for hospitals and health systems, and that small hospitals and underserved communities are disproportionately burdened. The same coverage also points out that many organizations need a repeatable, audit-ready credentialing file to prevent later enrollment defects, retroactive denials, and rework across payers, especially in anesthesia, radiology, ASCs, and multi-site physician platforms where one delayed or incomplete enrollment can suppress collections across a wider specialty panel, as described in Bristol Healthcare Services' credentialing guide.
Why this matters even beyond clean claims
Credentialing also shapes your advantage later. If a payer underpays, delays, or disputes a claim, your position is stronger when the provider file, enrollment history, and effective-date records are clean. Weak credentialing doesn't just hurt initial reimbursement. It also weakens the documentary foundation you need when payment issues escalate.
That's the fundamental frame. Credentialing is the first control point in revenue protection. If you build it like an administrative afterthought, the rest of the revenue cycle inherits the defect.
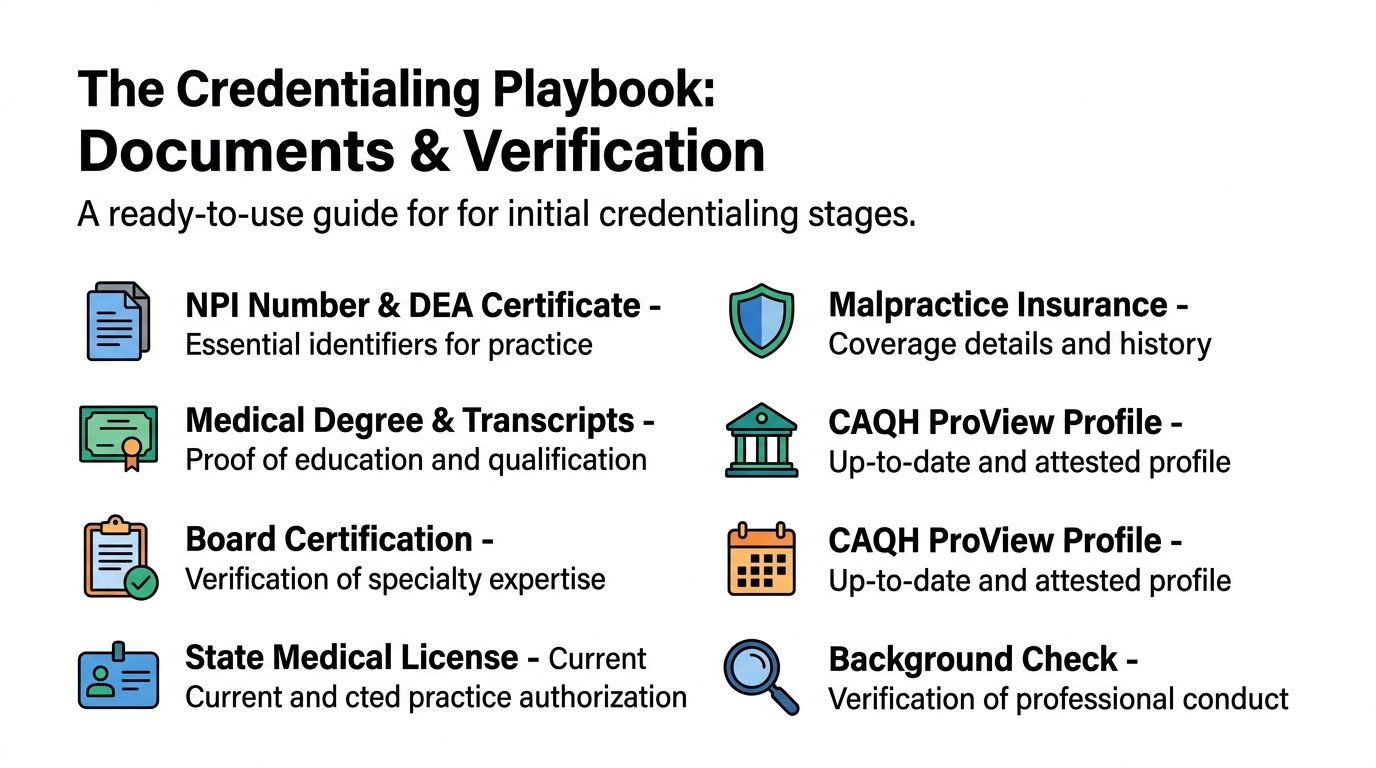
The Credentialing Playbook Documents and Verification
A solid provider credentialing process starts before the first payer form is touched. Most delays come from weak intake, not from some mysterious payer black box. If the provider file is incomplete, inconsistent, or assembled in the wrong order, everything downstream gets slower.
This visual is a useful checklist for the intake stage:
Build the file before you build the application
A high-control workflow follows a fixed sequence: pre-application document assembly, application submission, primary source verification, background and licensure review, committee review, privileging, and periodic recredentialing. That sequence also requires collecting licenses, board certifications, training records, work history, and government ID before submission, then confirming each item with the original issuer, as outlined in CapMinds' breakdown of the credentialing stages.
In practice, I want one complete provider packet that billing, credentialing, and leadership can all trust. At minimum, the file should include:
- Identity documents: Government-issued ID and legal name exactly as it should appear across payer and billing records.
- Licensure and authority to practice: State licenses, DEA where applicable, and any other practice authority documents relevant to the specialty.
- Education and training records: Medical degree, training completion documents, and board certification materials.
- Professional history: Current CV or resume with work history that is internally consistent and easy to validate.
- Insurance and risk documents: Malpractice coverage details and any supporting disclosures the payer may require.
- Core profile data: NPI information, practice locations, group affiliations, and a current CAQH ProView profile if your payer mix relies on it.
The key isn't collecting a pile of PDFs. The key is normalizing the data before submission. Dates should match across CV, applications, and source documents. Names should be consistent. Practice addresses should be final, not “temporary for now.”
A payer can overlook complexity. It rarely overlooks inconsistency.
Primary source verification is where control shows up
Primary source verification, or PSV, is what separates a credible file from a superficial one. You're not just accepting copies from the provider. You're confirming each credential with the original source.
That means the team should independently validate what matters most, such as:
- Licensure status with the issuing board
- Board certification with the certifying entity
- Education or training records with the original institution when required
- Professional history gaps or red flags through documented follow-up
- Current standing issues that could affect approval, privileging, or payer enrollment
If your staff is doing this manually, the process needs discipline. Every verification should be dated, saved, and easy to retrieve. If you're using a credentialing platform or outside support, the same rule applies. The system is only as good as the audit trail it produces.
What actually prevents rework
Teams often focus on form completion. Better teams focus on submission readiness. Before anything goes to a payer, I recommend a short internal review that checks three things:
| Control point | What to confirm | Why it matters |
|---|---|---|
| Data consistency | Names, dates, addresses, affiliations, and identifiers match across the file | Prevents avoidable discrepancy requests |
| Disclosure completeness | Work gaps, prior issues, and history questions are answered clearly | Reduces back-and-forth after submission |
| Billing alignment | Rendering setup, group linkage, and location details match expected claim configuration | Avoids post-approval claim defects |
If your front-end revenue team also handles patient intake, tie this work to medical eligibility verification workflows so payer setup, provider participation status, and front-desk expectations don't drift apart. Credentialing errors often surface at registration first, long before someone in finance sees the denial pattern.
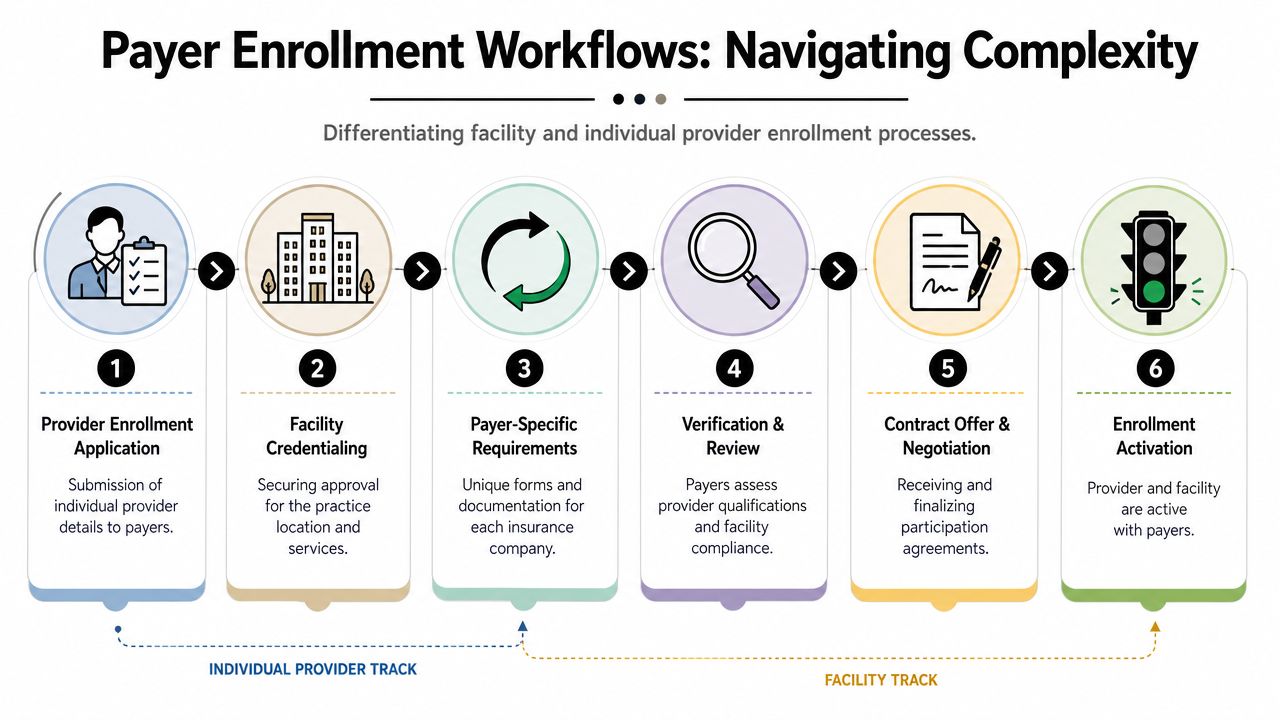
Navigating Complex Payer Enrollment Workflows
A provider starts seeing patients on Monday. By Friday, the front desk has verified benefits, the schedule is full, and claims are queued. Then billing finds out the clinician is credentialed but not enrolled correctly with two major payers at the right location and billing entity. The work was done, but the revenue is not collectible yet.
That is the operational gap between credentialing and enrollment. Credentialing confirms the provider is qualified. Enrollment determines whether the payer will recognize that provider, at that service address, under that tax ID and group, for payment. If any one of those elements is wrong, the denial shows up downstream.
The primary bottleneck is multiplicative risk
MedTrainer's overview of credentialing workflow complexity notes that providers, groups, and facilities often need enrollment with every accepted payer, averaging 5 to 10 payers per provider, group, or facility, which means one onboarding mistake can spread across several payer files at once, as described in MedTrainer's overview of credentialing workflow complexity.
That multiplier is what makes payer enrollment expensive to mishandle. One wrong suite number, practice start date, or group assignment can trigger a pending status with one payer, a rejection from another, and silent delay in a third portal. Staff then spend time correcting the same issue in different formats, under different tracking numbers, with different response rules.
The revenue impact is usually larger than the original error.
Here is how that plays out in day-to-day operations:
- One bad data element spreads everywhere: The same incorrect address, taxonomy, or effective date carries into multiple submissions.
- Each payer creates a different failure mode: One asks for a corrected attachment, one rejects the file outright, one pends it, and one gives no useful status update.
- Version control breaks down fast: Corrected forms end up in email chains, payer portals, shared drives, and scanned packets with no single authoritative copy.
- Billing gets conflicting status reports: One payer shows active, another still lists the provider as out-of-network, and another attached the provider to the wrong group or service location.
Facility and individual enrollment do not move together
Practice managers get burned when they assume facility approval covers the clinician, or that an enrolled clinician is automatically billable under the intended entity. Payers often treat those as separate decisions. Group linkage adds another layer, and it is the step many teams discover too late.
A simple comparison makes the risk clearer:
| Workflow | Main question | Common failure point |
|---|---|---|
| Individual provider enrollment | Is this clinician approved to participate and bill with this payer? | Mismatched provider data or incomplete disclosures |
| Facility credentialing | Is this location or entity approved for contracted services? | Missing entity-level documents or contract alignment issues |
| Group linkage | Is the approved provider properly attached to the right billing entity and service location? | Provider active on paper but not billable under the intended setup |
The most dangerous status in payer enrollment is “almost done.” That is when schedules fill, claims start dropping, and leadership assumes revenue is on the way even though reimbursement setup is still incomplete.
Controls that protect revenue
Practices that keep enrollment from turning into write-offs use production controls, not memory and email.
The minimum setup I recommend includes:
- A master payer matrix: Track payer name, enrollment type, submission date, reference number, current status, effective date, assigned owner, and missing items in one place.
- A single approved provider record: Maintain one governed source for provider demographics, affiliations, disclosures, identifiers, and location data before any application goes out.
- Payer-specific instructions: Document which payers require portal entry, which still accept paper, what attachments they ask for repeatedly, and how they handle corrections.
- Scheduled follow-up: Assign status checks by date and owner. Log every call, portal update, and reference number to prevent the file from stalling.
- Billing release criteria: Do not release a provider to billing until participation status, effective date, service location, and group linkage are confirmed against how claims will be submitted.
This work is administrative on the surface, but the outcome is financial. Clean enrollment determines whether claims pay at contracted rates, whether out-of-network exposure increases, and whether your team can defend underpayment or dispute activity later with a clear participation record. If enrollment data is sloppy, revenue cycle problems show up months after the application was submitted.
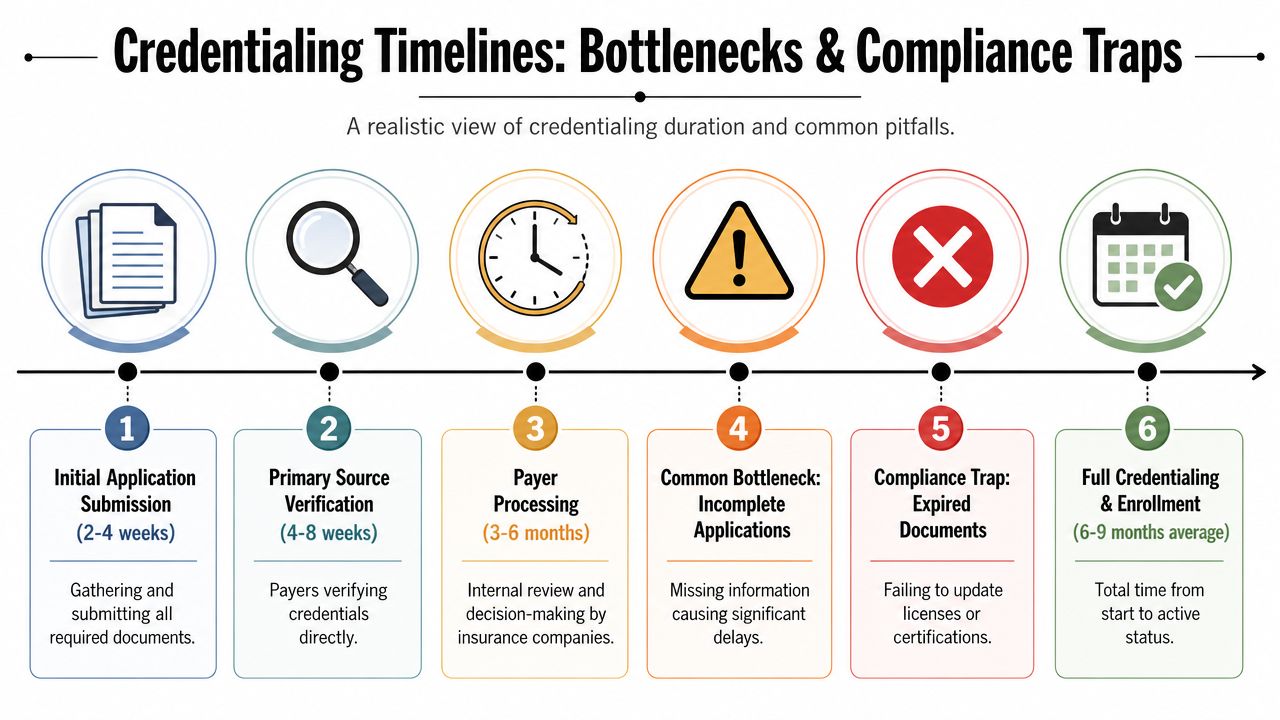
Timelines Common Bottlenecks and Compliance Traps
A lot of organizations still plan around an optimistic internal assumption that credentialing will wrap fast if everyone stays organized. That assumption usually fails when payer review starts.
Recent industry summaries report that most payer approvals take 60 to 180 days from submission to billing approval, and some materials also estimate 30 to 120 days depending on the organization and the completeness of primary source verification, according to ClinicMind's industry summary on provider credentialing timelines. The operational takeaway is simple: a newly hired clinician may wait months before the practice can bill under that provider's name.
The timeline below is closer to field reality than most optimistic internal rollout plans:
Where the process usually breaks
Delays rarely come from one dramatic event. They come from ordinary misses that stack up.
The most common bottlenecks I see are:
- Incomplete applications: Missing signatures, stale documents, unexplained work history, or conflicting dates.
- Slow discrepancy resolution: The provider doesn't answer follow-up questions quickly, or staff waits too long to chase missing items.
- Licensure and background review issues: Not necessarily adverse findings, but open questions that require manual clarification.
- Payer backlog: The file may be complete and still sit in queue without meaningful movement.
- Poor internal handoff: Credentialing is done working, but contracting, enrollment, and billing haven't aligned on what “done” means.
Compliance traps that create financial pain later
Some traps don't stop the application immediately. They create bigger problems after services have already been rendered.
Watch these closely:
Expired documents during review
A license, certificate, or insurance document can lapse while the application is pending. If the team doesn't refresh it before the payer asks, the clock resets in practice even if not formally.Incomplete disclosure handling
Prior malpractice matters, disciplinary history, or work gaps don't always cause denial. But poor explanation and weak documentation almost always create delay.Missed recredentialing triggers
Organizations often focus on the hire and forget that status maintenance is where preventable interruptions happen later.
Keep a live “expiring soon” list tied to every pending application. Static checklists go stale long before payer review does.
Plan for the delay you don't want
The right management question isn't “How fast can we finish?” It's “How do we protect revenue while the file is still moving?” That means controlling scheduling assumptions, setting clear provider start expectations, and separating clinical readiness from reimbursement readiness.
A practice that plans around best-case timing usually creates avoidable write-offs, delayed collections, or frustrated providers. A practice that plans around realistic timing protects cash and makes better staffing decisions.
Managing the Lifecycle Re-credentialing and KPIs
The provider credentialing process doesn't end at approval. It becomes a maintenance function the minute the provider goes live. Teams that treat it like a one-time onboarding task eventually lose status through neglect, not through complexity.
Credentialing has become more refined over the past 50 years, NCQA standards require primary-source checks, and provider privileges are typically reviewed every 2 years. Other industry guidance commonly places recredentialing on a 2 to 3 year cycle, as summarized in the StatPearls review of medical staff credentialing. That means your operating model has to support recurring review, document refresh, and status monitoring.

Recredentialing is an operations discipline
The organizations that stay out of trouble don't wait for notices. They maintain a live inventory of provider records, renewal dates, payer participation status, and committee review cycles. That work belongs in the same management rhythm as denials, aging, and collections.
A practical recredentialing cadence includes:
- Document surveillance: Track upcoming expirations for licenses, insurance, certifications, and any payer-required records.
- Profile maintenance: Keep provider demographic and affiliation data current when locations, supervisors, or group structures change.
- Status reconciliation: Compare internal records against payer rosters and billing setup to catch silent mismatches.
- Committee and privileging calendar control: Make sure facility-side reviews don't drift away from payer-side maintenance.
- Exception handling: Flag providers with prior issues, multi-state complexity, or specialty-specific enrollment dependencies for closer follow-up.
The KPIs worth measuring
If you don't measure credentialing, it gets managed by anecdotes. The better approach is to run it like a revenue-supporting production process and connect it to broader revenue cycle optimization efforts.
I'd track a small set of KPIs consistently:
| KPI | What it tells you | Why it matters |
|---|---|---|
| Time to submit | How long it takes to assemble a complete file and get it out the door | Shows intake efficiency and provider responsiveness |
| Time to effective date | How long until the provider is truly billable | Connects credentialing work to revenue activation |
| First-pass application success rate | How often submissions avoid correction cycles | Measures file quality, not just staff effort |
| Credentialing-related denial rate | How many denials trace back to enrollment or provider setup defects | Exposes downstream leakage from front-end failures |
| Recredentialing completion before due date | Whether maintenance work is proactive or reactive | Reduces avoidable participation gaps |
If a team celebrates submission volume but can't report effective dates and denial patterns, it isn't managing credentialing as a business process.
What good looks like
Good credentialing operations are boring in the best sense. Files are complete. Dates are tracked. Follow-up is documented. Billing knows exactly when a provider is active and under which payer configuration. Leadership can see where revenue is pending and why.
That's the shift that matters. Credentialing stops being a hidden admin burden and becomes a monitored control system with visible financial consequences.
When to Escalate to a Specialist Partner
A common inflection point looks like this. The provider is hired, scheduled, and clinically ready, but claims cannot go out cleanly because payer enrollment is still pending, records do not match across systems, or no one can pin down the effective date. At that stage, credentialing is no longer an admin workload issue. It is a cash delay with staffing and forecasting consequences.
Practices usually feel this first in revenue, not compliance. Days in A/R rise for a new provider cohort. Enrollment defects show up as avoidable denials. Finance gets asked when a provider will start producing, and the answer is still "we're waiting on the payer." QGenda's guide discusses the typical credentialing and payer enrollment window as a lengthy process that can stretch for months, especially when payer approvals lag or panels are closed, in its guide to provider credentialing and payer enrollment.
Signals that in-house control may not be enough
Specialist support makes sense when the problem is no longer just workload, but process reliability and revenue exposure.
- You're adding providers faster than your team can activate them: Hiring success does not help if enrollment delays keep those visits off the books or out of network.
- You're expanding across states or tax IDs: More entities, licenses, and payer rules create enough variation that manual tracking starts to break.
- You're in a specialty with higher payer friction: Anesthesia, radiology, ASC models, hospital-based groups, and emergency-adjacent services often require tighter coordination across locations, rosters, and contracts.
- Denials trace back to provider setup or participation status: Once billing is correcting credentialing defects after claims submission, the cost is already higher.
- Your team cannot produce a clean active-by-payer roster: If leadership cannot see who is billable, where, and under which contract, revenue forecasting is guesswork.
- Recredentialing work is driven by last-minute notices: That usually means deadlines are being managed by payer reminders instead of your own controls.
What a specialist partner should improve
A good partner improves speed, but speed alone is not the point. The primary measure is whether they reduce revenue leakage. That means cleaner intake, fewer correction cycles, documented payer follow-up, accurate roster management, and clear handoffs to billing so claims are held or released based on verified status, not assumptions.
They should also strengthen your position when reimbursement disputes show up later. If provider enrollment dates, participation records, and payer communications are incomplete, underpayment reviews and IDR preparation get harder than they need to be. Clean credentialing records help establish when a provider was eligible to bill, under which entity, and with what network status.
Outsourcing fails when it creates a black box between operations, credentialing, and billing. It works when the partner gives your team better visibility, tighter controls, and a process you can audit. If that is the gap you need to close, review specialized credentialing services with the same standard you would apply to any revenue protection function.
If your staff spends too much time chasing payer updates, fixing enrollment defects, or explaining delayed provider cash to leadership, bringing in a specialist is a practical move. The right partner should lower denials, shorten the path to billable status, and give the revenue cycle team a cleaner starting point.