
Your practice may be busier than ever and still feel financially weaker than it did a few years ago. Schedules are full. Providers are productive. The phones don't stop. Yet cash arrives late, denials keep stacking up, and payer reimbursements don't match the value of the care delivered.
That isn't a billing-office problem. It's an enterprise value problem.
If you're a physician owner, operator, or private equity partner, you should stop thinking about revenue cycle optimization as a narrow collections function. The job is broader. You need a system that protects revenue from the first patient touch through final payment enforcement. Anything less leaves money on the table for payers to keep.
Why Revenue Cycle Optimization Is Your Practice's Lifeline
A lot of practices make the same mistake. They see revenue cycle optimization as a cleanup exercise. Claims go out, denials come back, staff rework them, and leadership hopes collections stabilize. That model is obsolete.
The modern payer environment punishes reactive organizations. A practice can deliver strong care, maintain solid patient demand, and still lose margin because the administrative path to payment is broken. Registration errors start the slide. Eligibility misses create avoidable denials. Coding inconsistency weakens claims. Payment posting hides underpayments. Then leadership asks the billing team why cash is tight.
The problem isn't volume
High volume can mask operational weakness for a while. It can't fix it.
What matters is whether the organization converts documented care into timely, defensible, fully reconciled payment. That's what revenue cycle optimization means. It's a strategic discipline that connects front desk operations, coding, credentialing, claim quality, denial management, payer behavior, and payment enforcement.
Clean claims are necessary. They are not sufficient.
That distinction matters. A claim can be technically correct and still be delayed, downcoded, or underpaid. If your operating model stops at “submit and follow up,” you've built a billing process, not a revenue protection system.
Why this matters to investors and operators
Private equity-backed platforms should care because fragmented RCM creates hidden earnings erosion. Specialty groups should care because complexity increases payment risk. Hospitals and ASCs should care because every breakdown in the cycle raises labor cost and slows cash conversion.
The practices that outperform don't treat RCM as back-office plumbing. They treat it like a core operating capability. They design workflows that produce clean, dispute-ready claims upstream and preserve the evidence needed downstream if payers don't honor the claim appropriately.
That's the integrated RCM and IDR model. It's not a niche tactic. It's where serious revenue cycle optimization is headed because collections alone no longer close the loop.
Mapping the Healthcare Revenue Lifecycle
Think of the revenue cycle as a financial supply chain. Every handoff affects the value of what reaches the end. If one upstream input is weak, the final reimbursement outcome deteriorates.
The cycle starts before care is delivered
Patient access is where many organizations lose control early. Registration, insurance capture, eligibility verification, benefit checks, prior authorization, and provider credential alignment all happen before a claim exists. If your team gets these wrong, the downstream billing staff inherits a preventable mess.
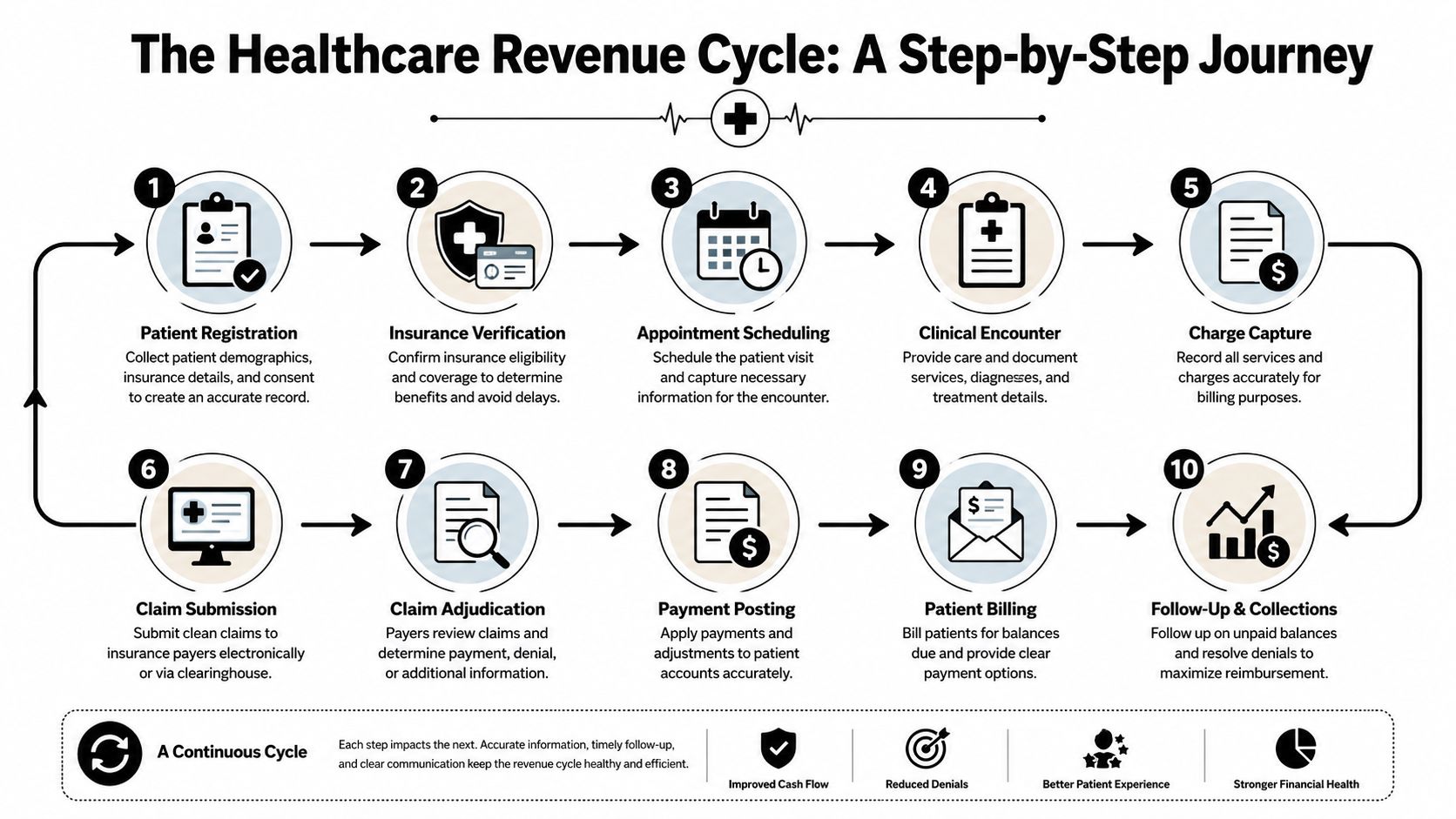
A workable sequence looks like this:
- Patient registration captures accurate demographic and insurance data.
- Eligibility verification confirms active coverage and identifies plan-specific requirements.
- Authorization and referral control validates medical necessity pathways where required.
- Credentialing alignment ensures the rendering and billing entities match payer enrollment rules.
If you want a plain-language view of how payers evaluate submitted claims, study the claim adjudication process. It clarifies why errors that seem minor at intake often turn into delayed or reduced payment later.
Mid-cycle work determines claim quality
After care is delivered, charge capture and coding decide whether the claim accurately reflects services rendered. At this juncture, clinical documentation integrates with reimbursement logic.
The core activities include:
- Charge capture discipline: Services need to be captured completely and matched to the encounter.
- Coding accuracy: Diagnosis and procedure coding must support medical necessity and payer edits.
- Claim scrubbing: Edits should catch formatting, policy, and coding conflicts before submission.
- Timely submission: Lag kills collections and weakens appeal power.
The back end is more than posting payments
The back end is often defined too narrowly. Posting payments is only one part of it. You also need denial classification, appeals, patient balance resolution, contract compliance review, and final reconciliation against what should have been paid.
Every stage in the cycle either strengthens the claim or weakens your ability to defend it later.
A complete lifecycle includes these closing stages:
| Stage | What it does |
|---|---|
| Payment posting | Records remittances and adjustments accurately |
| Denial management | Separates correctable denials from payer-driven friction |
| Patient collections | Resolves legitimate patient responsibility without creating avoidable write-offs |
| Reconciliation | Compares actual payment to expected reimbursement and flags variances |
| Enforcement | Escalates underpayments and disputes when ordinary follow-up won't fix the issue |
That final step is where many organizations still stop short. They map the process to collections, not to recovery of full value. That's a costly blind spot.
Where Your Revenue Is Leaking and How to Find It
Revenue leakage rarely comes from one dramatic failure. It comes from repeated small misses that leadership tolerates because each one looks operational rather than strategic.
Specialty practices are especially exposed. The leakage pattern in orthopedics doesn't look like the leakage pattern in anesthesia. Air ambulance doesn't break in the same places as gastroenterology. If you use one generic denial workqueue for all of it, you're hiding the problem instead of fixing it.
Leakage is specialty specific
Here's where the weak points usually sit:
| Specialty | Front-End Leakage (Pre-Submission) | Back-End Leakage (Post-Adjudication) |
|---|---|---|
| Orthopedics | Procedure coding complexity, documentation gaps, authorization errors | Downcoding, reduced reimbursement on high-value procedures, missed appeal opportunities |
| Anesthesia | Modifier misuse, time documentation inconsistency, credentialing mismatches | Payment variance tied to unit calculation disputes and payer interpretation |
| Air ambulance | Incomplete transport documentation, medical necessity support gaps | Aggressive payer underpayment, dispute escalation failures, unsupported adjustments |
| Gastroenterology | Prior authorization breakdowns, site-of-service rule misses | Denials tied to policy edits, payment shortfalls after adjudication |
| Dermatology | Charge capture inconsistency, coding variation across providers | Bundling issues, reduced payment on procedural claims |
| Radiology | Order and documentation mismatch, exam coding errors | Technical and professional component payment discrepancies |
The point isn't that every practice has every problem. The point is that each specialty has predictable failure modes. Your workflow needs to reflect them.
Denials are pattern problems
Denials aren't random. They cluster by payer policy, code combinations, documentation patterns, and patient demographics, which is why analytics and automation now play a central role in identifying bottlenecks, strengthening eligibility verification, improving claims submission, and scoring claims before submission, as outlined in this healthcare revenue cycle optimization guidance from Experian.
That changes how competent operators should work. Don't wait for remits to tell you where the problem was. Score risk before the claim goes out. Segment denials into front-end preventable issues versus post-adjudication payer behavior. Then redesign the workflow based on those cohorts.
Practical rule: If your denial team can describe denial categories but can't trace them back to specific intake, coding, or payer-rule failures, you don't have root-cause management.
A few examples of useful analysis:
- Pre-bill risk scoring: Flag claims likely to deny based on payer edits, code combinations, and documentation gaps.
- Underpayment detection: Compare actual reimbursement against the insurance allowed amount and expected contract logic.
- Payer clustering: Separate one-off errors from systematic payer behavior.
- Provider variation review: Identify physicians or locations with recurring documentation or coding drift.
Where to look first
Most organizations already have the raw material. The issue is focus.
Start with these questions:
- Which denial reasons repeat by payer? Repetition means process failure or payer strategy.
- Which specialties generate the most manual rework? Labor concentration usually signals claim design weakness.
- Where are adjustments growing without clear justification? That often points to underpayment or reconciliation failure.
- Which claims become hard to defend later? Those are the claims that weren't built to be dispute-ready in the first place.
You don't need more dashboards. You need sharper operational segmentation and the discipline to act on it.
The KPIs That Truly Measure Financial Health
Most KPI decks are bloated. They produce motion, not control. A leadership team doesn't need dozens of indicators. It needs a short list that reveals cash conversion, claim quality, and operational efficiency.
The core metrics worth managing
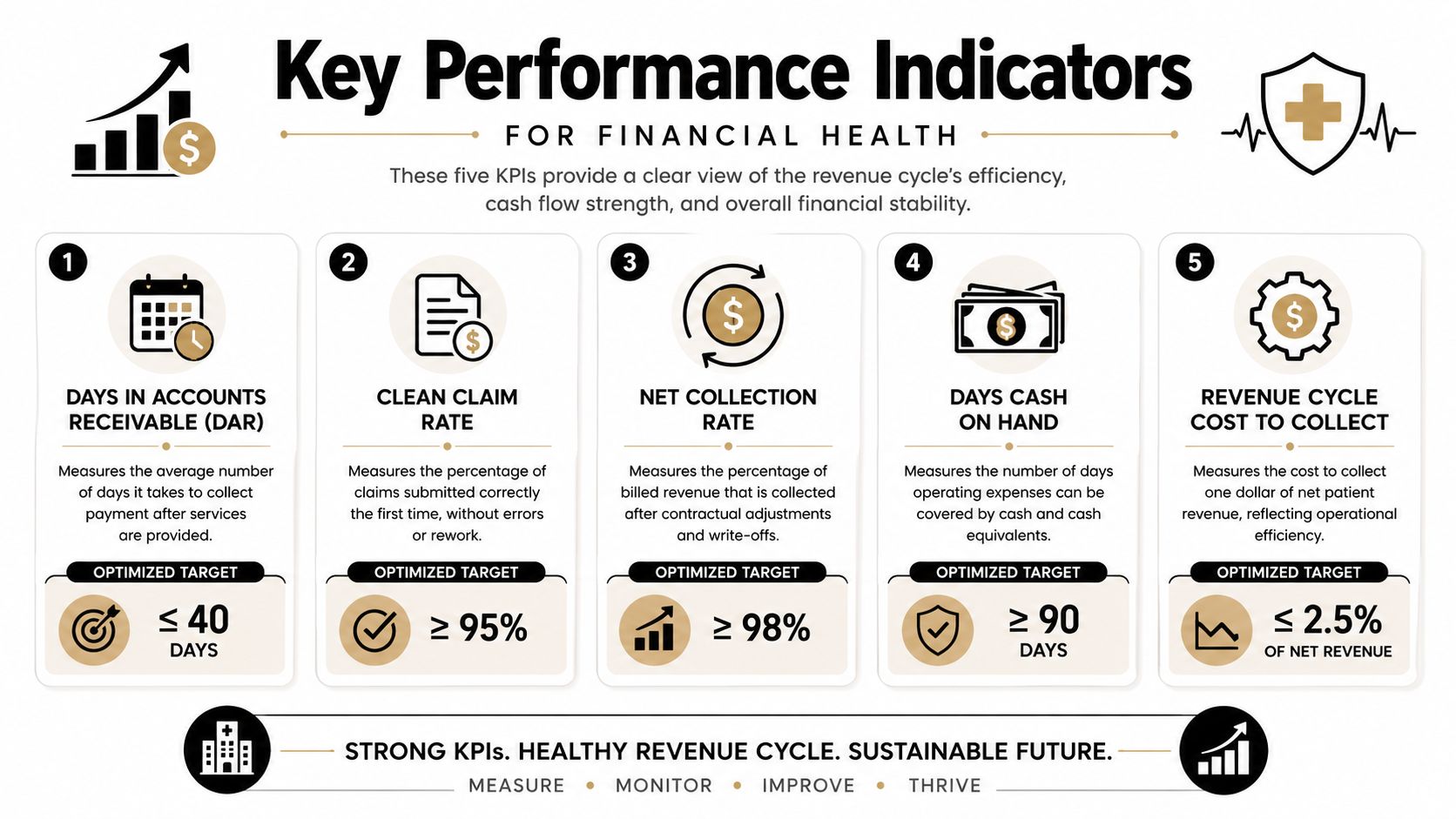
Leading benchmarks track days in accounts receivable at 40 days or less, clean-claim rates at 90% or higher, and cost to collect at 3 to 4 percent or lower, according to MD Clarity's revenue cycle optimization benchmark summary. Those aren't vanity numbers. They tell you whether the operation is converting work into cash efficiently.
Use them this way:
| KPI | What it tells you |
|---|---|
| Days in A/R | Whether cash is moving or getting trapped in the system |
| Clean-claim rate | Whether the front and middle of the cycle are producing submission-ready claims |
| Cost to collect | Whether labor and process overhead are consuming too much reimbursement |
| Denial rate | Whether preventable friction is entering the cycle |
| Net collection ratio | Whether the organization is capturing the reimbursement it has earned |
What good management looks like
The mistake is reporting these metrics passively. Good operators tie each KPI to a person, a workflow, and a corrective action.
For example, a weak clean-claim rate isn't a billing-office embarrassment. It's evidence that patient access, coding, documentation, or edits are failing upstream. Rising A/R isn't “just collections.” It often means avoidable denials, slow follow-up prioritization, or unresolved payer variance is stacking up.
A few well-chosen KPIs will tell you more than a monthly packet full of operational trivia.
If you're at the executive level, ask for three things from every KPI review:
- Root cause mapping: What operational behavior drove the number?
- Ownership: Which leader owns the fix?
- Time-bound action: What changes before the next reporting cycle?
That's how KPIs become management tools instead of meeting decoration.
Building Your RCO Engine People Process and Technology
You don't improve revenue cycle performance by buying software and hoping the team adapts. You improve it by building an operating engine where people, process, and technology reinforce each other.
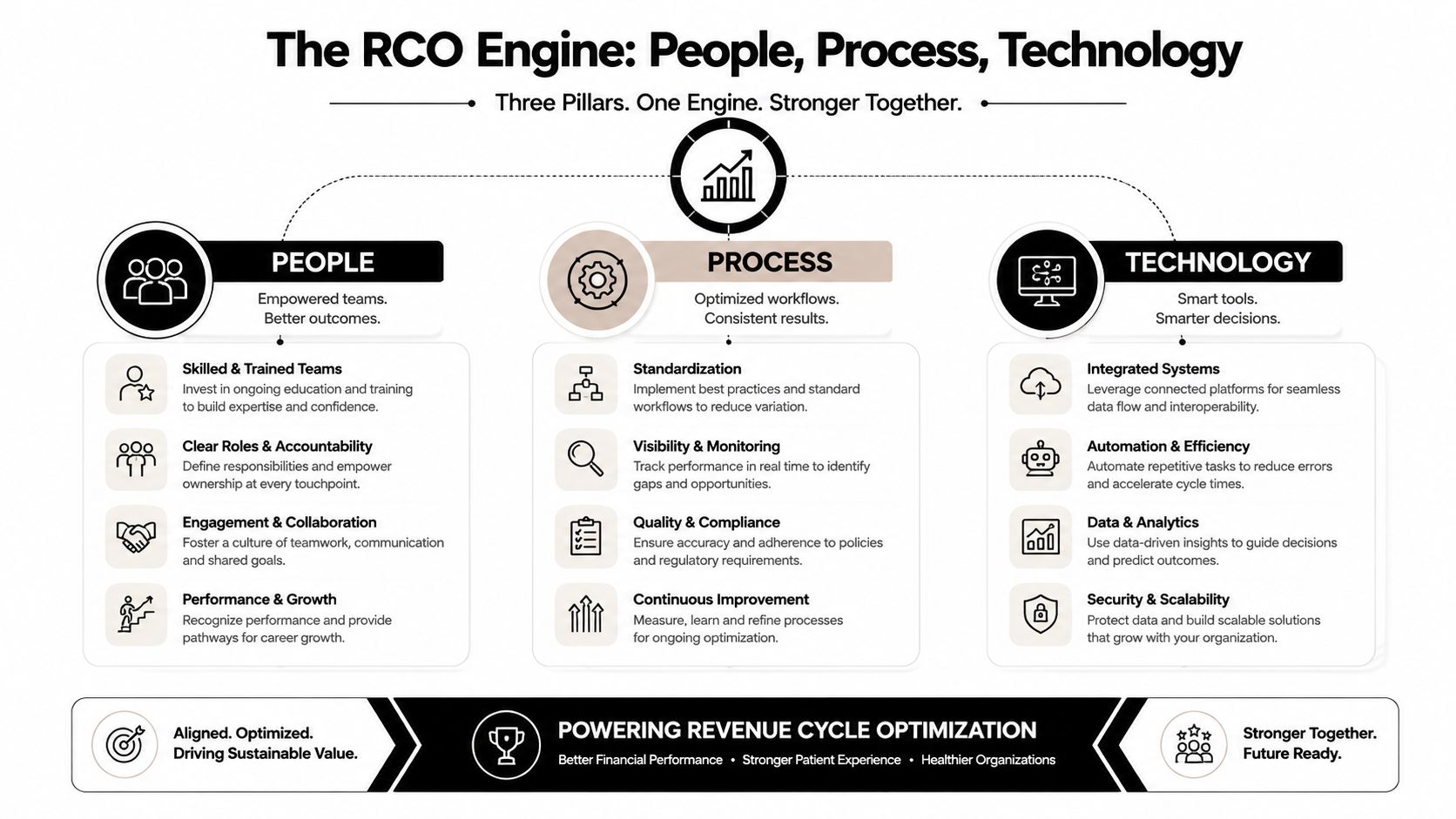
People need accountability, not just effort
Most RCM teams are working hard already. Hard work isn't the issue. Role clarity is.
Front desk staff should own data accuracy and eligibility discipline. Coding leaders should own documentation feedback loops. Denial teams should separate recoverable technical errors from payer conduct issues. Finance should own reconciliation, not just posting. If everyone “touches” the revenue cycle but nobody owns handoff quality, leakage becomes permanent.
Useful people practices include:
- Defined ownership: Assign accountability by stage, not by vague department label.
- Specialty training: Teach teams the payer and coding risks unique to their service lines.
- Escalation rules: Decide early which issues are routine rework and which require enforcement posture.
Process should produce dispute-ready claims
A strong process does more than move claims faster. It preserves the evidence trail needed if payment is contested later.
That means your workflows should require complete intake documentation, credential consistency, accurate coding support, claim edit resolution, payment variance review, and disciplined appeal packaging. If these live in disconnected teams with inconsistent standards, your downstream advantage is lost.
One practical way to rebuild process is to map each failure into one of three categories:
- Preventable front-end defects
- Correctable submission and follow-up errors
- Payer-driven underpayment or adverse adjudication
That framework forces the organization to stop treating all payment friction as the same problem.
Technology should reduce routine labor
AI and automation now sit at the center of revenue cycle optimization, with one industry source stating that these capabilities could realize up to $360 billion in annual savings across healthcare through predictive analytics, automated eligibility checks, and digital claim workflows, as noted in this healthcare automation overview from Heidi Health.
That doesn't mean replacing staff. It means redeploying them toward exceptions, analysis, and recovery.
The right technology stack handles repetitive validation early so skilled staff can focus on denials, underpayments, and contract variance.
Prioritize technology that supports:
- Eligibility automation
- Pre-bill claim scoring
- Rules-based claim scrubbing
- Payment variance detection
- Payer behavior dashboards
Some organizations build this in-house. Others use specialized vendors. For groups that need an integrated operating model, RevGuard's medical collections software approach sits in the category of tools that connect RCM workflow, collections, analytics, and downstream enforcement logic rather than treating them as separate systems.
Closing the Loop with Enforcement Driven IDR
Conventional RCM thinking says the cycle ends when the claim is paid or written off. That's exactly where too many organizations lose their advantage.
A clean claim doesn't guarantee a proper outcome. Payers can still delay, downcode, reclassify, or underpay. If your team has no structured enforcement model after adjudication, you've trained the payer that friction works.
Why enforcement belongs inside optimization
Independent Dispute Resolution under the No Surprises Act shouldn't be treated as a rare legal side path. In the right cases, it is the final operational step in revenue cycle optimization.
That changes the design of the whole cycle. Registration has to be accurate. Documentation has to support acuity and medical necessity. Coding has to be precise. Payment posting has to surface variances cleanly. Reconciliation has to distinguish ordinary undercollection from dispute-worthy underpayment. When those pieces are built correctly, the claim becomes dispute-ready.
What dispute-ready actually means
A dispute-ready claim includes the operational evidence needed to support payment enforcement. Not just the billed amount. The full record.
That usually means:
- Clean intake data that supports coverage and patient status
- Complete documentation that matches the service delivered
- Coding logic that survives scrutiny
- Credentialing alignment that avoids technical attack points
- Payment analysis showing where adjudication diverged from expected value
The strongest IDR strategy starts long before arbitration. It starts when the claim is built.
For investor-backed platforms, this demands attention. If you separate upstream RCM from downstream dispute strategy, you create a break in the evidence chain. Operations optimize for speed. Legal or arbitration teams inherit weak files. Recovery suffers.
The integrated model is the new standard
The integrated RCM and IDR model fixes that break. It treats upstream claims work as preparation for both reimbursement and enforcement. It also treats downstream dispute outcomes as feedback that should reshape coding rules, documentation standards, and payer targeting.
That's why this approach is becoming the new standard of care for revenue protection. It recognizes payer behavior as part of the operating environment, not as an occasional exception. And it gives the organization a way to defend reimbursement value instead of merely requesting it.
Your Roadmap Quick Wins and Long Term ROI
You don't need a grand transformation memo. You need a sequence.
Quick wins in the first stretch
Start with the issues that create immediate friction:
- Tighten eligibility checks: Fix registration discipline, coverage validation, and authorization capture before service.
- Scrub recurring denial drivers: Pull your top repeat edits and force pre-submission resolution.
- Audit payment variances: Review remittances for underpayment patterns instead of posting and moving on.
- Standardize specialty workflows: Orthopedics, anesthesia, GI, and emergency services should not share one generic denial playbook.
These changes are usually operational, not philosophical. That's why they move fast.
Stabilization after the first push
Once the obvious leaks are addressed, lock in management control.
Use a small KPI set. Assign ownership by stage. Separate front-end defects from payer-driven reimbursement behavior. Build a routine where revenue cycle leaders, finance, and operational leadership review the same facts and make decisions from them.
A strong stabilization period also includes documenting which claims should be preserved for escalation, not just reworked in standard queues.
Long-term optimization creates durable ROI
The long-term payoff comes from integration. Payer behavior analytics should inform claim design. Underpayment findings should shape contract review. IDR outcomes should feed back into documentation standards and specialty training. That's how revenue cycle optimization becomes a compounding capability instead of a recurring cleanup effort.
If your team only measures collections, it will miss the reimbursement value payers never intended to hand over voluntarily.
The practices and platforms that outperform will be the ones that operate with an enforcement mindset. They won't just accelerate cash. They'll protect earned revenue all the way through final resolution.
If your organization needs a tighter revenue protection model, RevGuard offers an integrated approach that connects specialty-specific RCM with enforcement-driven IDR under the No Surprises Act. That structure fits providers and multi-site platforms that need cleaner claims upstream, clearer payer intelligence in the middle, and a formal path to recover underpayments when ordinary collections won't get there.