A rejected 58100 claim usually doesn't start with a dramatic coding mistake. It starts with something small. The clinician documents abnormal bleeding but doesn't clearly state the indication for biopsy. The procedure note says tissue was obtained, but never says the cervix was not dilated. Or the same-day E/M gets added automatically, and nobody checks whether the documentation supports a separate service.
That's how revenue leaks in gynecology. Not through rare edge cases alone, but through routine encounters billed as if the code definition is enough.
For an office endometrial biopsy, the code itself is straightforward. The problem is that payers don't reimburse the definition. They reimburse the documented service, matched to a covered diagnosis, submitted without bundling conflicts, and defended when edits hit. If any one of those pieces is weak, a clean clinical encounter turns into rework, write-offs, or a preventable appeal.
I've seen new billers focus too much on the procedure name and not enough on the operational decision points that decide payment. Endometrial biopsy coding is one of those areas where the unwritten rules matter as much as the descriptor. Cervical dilation changes everything. Included services get unbundled by mistake. Same-day E/M visits are overbilled or underbilled. Failed attempts sit in charts with vague notes that don't support any clear claim strategy.
Introduction The Cost of a Simple Coding Error
A common workflow failure looks like this. The provider sees a patient for abnormal uterine bleeding, performs an office biopsy, and the claim goes out with CPT 58100. A few days later, the payer rejects it. The denial reason points to medical necessity, bundling, or modifier conflict. The chart gets pulled. The team realizes the note never clearly tied the diagnosis to the procedure, or it suggested a more complex encounter than the code submitted.
That single denial isn't the true cost. The true cost is staff time spent reopening the chart, querying the provider, correcting the claim, monitoring the resubmission, and deciding whether the payer's edit is legitimate or worth fighting. When that pattern repeats across a high-volume gynecology service line, it becomes a revenue protection problem, not just a coding problem.
Where practices usually get burned
The trouble spots are predictable:
- Missing medical necessity linkage: The diagnosis is present somewhere in the chart, but not cleanly tied to the biopsy decision.
- Procedure note gaps: The note confirms sampling but doesn't make clear whether cervical dilation occurred.
- Same-day E/M confusion: Staff add an E/M code because there was a visit, but the documentation only supports the work inherent to the procedure.
- Borderline procedural scenarios: The provider attempted a standard biopsy, encountered stenosis, altered the technique, and documented the whole event in a way that leaves coding open to interpretation.
Practical rule: If a claim for an endometrial biopsy looks simple, that's the moment to slow down and check the note. Straightforward gynecology claims often deny for routine reasons that could have been prevented before submission.
The way to protect revenue isn't to memorize one CPT code. It's to understand where the claim changes category, what documentation locks in the correct code, and how to submit the encounter so it's defensible if the payer challenges it.
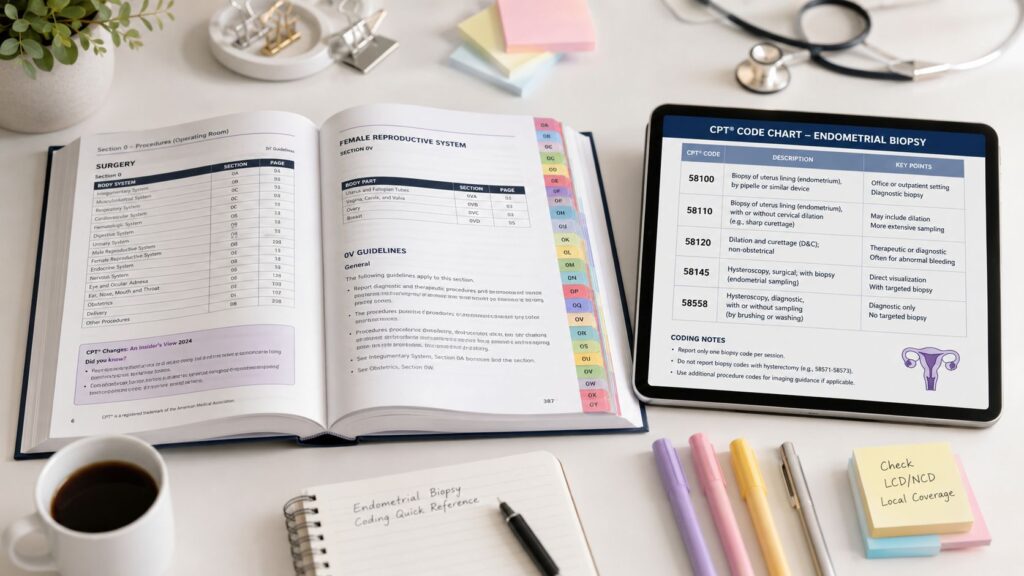
CPT 58100 The Core Endometrial Biopsy Code
A payer denial often starts with a note that says “endometrial biopsy performed” and nothing more. The biller sees 58100, submits the claim, and then the problem shows up later: the provider also documented cervical stenosis, difficulty passing the instrument, or a same-day workup that may or may not support a separate E/M. That is why 58100 has to be treated as a narrow code with clear limits.
CPT 58100 reports endometrial sampling, with or without endocervical sampling, without cervical dilation. That last phrase does the heavy lifting. It tells you what is bundled into the code and, just as important, what pushes the case out of 58100 and into a different coding path.
What 58100 includes in the real world
For routine office or outpatient diagnostic sampling, 58100 is usually the correct starting point. It covers the biopsy session itself. If the clinician also performs endocervical sampling during that encounter, that work is included. It does not include the pathology interpretation, and it should be reported once per session, not by number of passes.
Those details affect revenue in predictable ways:
- Do not bill multiple units because the provider made more than one pass to obtain tissue.
- Do not carve out endocervical sampling if it occurred as part of the same biopsy encounter.
- Do not force pathology into 58100. Tissue collection and pathology reading are separate services.
- Check the global implications before adding follow-up services tied to routine post-procedure care.
Teams that struggle with these distinctions usually do not have a codebook problem. They have a workflow problem. A specialty-specific medical coding review process for gynecology claims helps catch the note details that determine whether 58100 is defensible before the claim goes out.
Where 58100 stops
The denial risk sits at the border cases.
If the physician performs a standard office biopsy and obtains tissue without dilation, 58100 is the core code. If the record shows cervical dilation and the service becomes a D&C, 58100 is no longer the safe choice. That is the scenario where billers get burned by assuming every uterine sample belongs under the same code.
Failed attempts create a separate problem. If the provider attempted the biopsy but could not obtain a sample, billing 58100 depends on what was completed and how the payer treats unsuccessful procedures. Do not guess from the scheduling label or the order. Read the procedure note line by line. Revenue protection starts there, because an avoidable denial costs more than the original charge correction.
The questions I want answered before 58100 goes on a claim
| Review point | What supports 58100 | What should trigger a second review |
|---|---|---|
| Was endometrial tissue actually sampled? | Clear statement that sampling was performed | Attempt documented, but no specimen obtained |
| Was the service diagnostic endometrial biopsy work? | Routine office or outpatient biopsy note | Procedure escalated beyond standard sampling |
| Did the note confirm no cervical dilation? | Technique supports passage without dilation | Stenosis, dilation, or more extensive intervention documented |
| Was endocervical sampling done too? | Still included in 58100 | Staff tries to bill it separately |
| Is pathology billed by another entity? | Expected and separate | Team tries to append pathology work to 58100 |
A strong biller reads 58100 as a code with edges. The claims that pay cleanly are the ones where the documentation shows exactly why the case stayed inside those edges.
Required Documentation for a Denial Proof Claim
A denial-proof 58100 claim is built in the chart before the claim ever drops. I have seen clean procedures deny because the note left one gap: no stated indication, no specimen disposition, or no clear record of whether the cervix required dilation. Once the payer sees ambiguity, the burden shifts to your team to prove what happened after the fact. That is expensive rework, and it is exactly the kind of revenue leakage RevGuard is meant to prevent.
What the chart has to prove
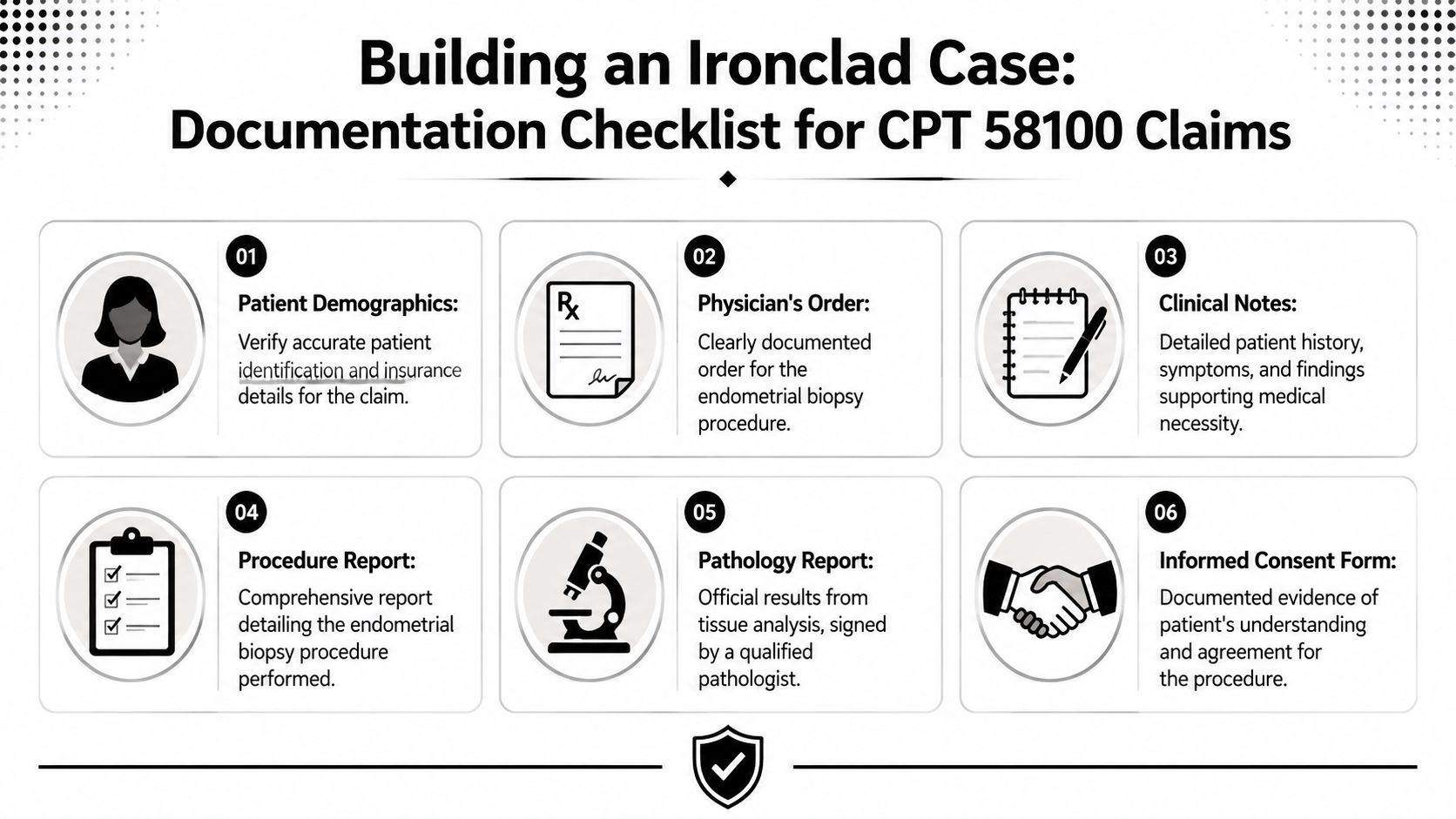
For an endometrial biopsy CPT claim to hold up under review, the record should answer five payer questions clearly:
- Why was the biopsy medically necessary? The presenting symptom, failed prior treatment, imaging concern, or surveillance reason should be stated plainly.
- What did the clinician evaluate before proceeding? History, exam findings, prior test results, and risk factors should support the decision to biopsy.
- What procedure was completed? The note should identify endometrial sampling and describe the technique used in terms that match the service billed.
- Was tissue obtained and what happened to it? If a specimen was collected, the note should show that it was sent to pathology or otherwise handled appropriately.
- Was informed consent documented? Payers do not always ask for it on the first pass, but missing consent weakens an appeal file.
One line can determine whether 58100 pays or stalls. The procedure note should make clear that the biopsy was performed without cervical dilation, or at minimum describe the technique in a way that leaves no doubt. If the note mentions stenosis, difficult entry, or mechanical widening of the cervix and never resolves that detail, expect edits, requests for records, or a code challenge.
What I audit before releasing the claim
A biller should be able to confirm these items without guessing:
- The indication is explicit. “Abnormal uterine bleeding,” “postmenopausal bleeding,” “thickened endometrium on ultrasound,” or another documented reason should appear in the assessment and support the diagnosis coding.
- The procedure note stands on its own. Do not rely on scattered language in the office note to explain the biopsy.
- The technique is specific enough to defend the code. Include how the uterus was accessed, whether the cervix was traversed without dilation, and whether tissue was obtained.
- Specimen handling is documented. Collection and submission belong in the procedure record, even though the pathology interpretation is billed separately.
- Failed attempts are easy to identify. If no sample was obtained, the note should say that directly instead of implying a completed biopsy.
- Any same-day E/M work is separately supported. A distinct problem, separate decision-making, or management beyond the usual pre-procedure work should be obvious in the record.
The highest-value habit is reading for denial risk, not just code selection. A note that says “endometrial biopsy attempted” is not the same as a note that says tissue was obtained and sent. A note that says “cervix stenotic, dilator used” creates a very different coding path than a routine office biopsy. Those are the what-if details that protect revenue. If they are missing, hold the claim, query the provider, and fix the chart before submission.
Mapping ICD-10 Diagnosis Codes for Medical Necessity
Payers don't review a CPT code in isolation. They test whether the diagnosis on the claim makes the procedure clinically reasonable. With an endometrial biopsy, that means your ICD-10 selection has to reflect the symptom, suspected pathology, or clinical concern that drove the biopsy decision.
The clinical rationale for this is strong. A major evidence review summarized that the Pipelle technique had 81% sensitivity, and the specificity of all devices exceeded 98% for detecting endometrial carcinoma and atypical hyperplasia. The same review also noted that cervical cytology was a much weaker proxy, with a positive predictive value of only 13% to 17% for endometrial malignancy when endometrial cells were seen on cervical cytology, according to Aetna's clinical policy bulletin on endometrial biopsy evidence. That's why biopsy remains a foundational office diagnostic tool for abnormal or postmenopausal bleeding.
Common ICD-10 codes supporting CPT 58100
Use the diagnosis that best reflects the documented reason for the procedure. Don't code from habit. Code from the chart.
| ICD-10 Code | Description | Category |
|---|---|---|
| N95.0 | Postmenopausal bleeding | Bleeding symptom |
| N93.8 | Other specified abnormal uterine and vaginal bleeding | Bleeding symptom |
| N92.0 | Excessive and frequent menstruation with regular cycle | Menstrual abnormality |
| N92.1 | Excessive and frequent menstruation with irregular cycle | Menstrual abnormality |
| N92.4 | Excessive bleeding in the premenopausal period | Menstrual abnormality |
| N92.6 | Irregular menstruation, unspecified | Menstrual abnormality |
| N85.00 | Endometrial hyperplasia, unspecified | Endometrial pathology |
| N85.01 | Benign endometrial hyperplasia | Endometrial pathology |
| N85.02 | Endometrial intraepithelial neoplasia [EIN] | Endometrial pathology |
| N84.0 | Polyp of corpus uteri | Uterine pathology |
| C54.1 | Malignant neoplasm of endometrium | Malignancy |
| D07.0 | Carcinoma in situ of endometrium | Malignancy |
| N97.2 | Female infertility of uterine origin | Infertility evaluation |
| N97.0 | Female infertility associated with anovulation | Infertility evaluation |
What works and what gets flagged
A diagnosis supports payment when it matches the provider's narrative. A patient with postmenopausal bleeding and a biopsy performed to evaluate endometrial pathology is a coherent claim. A vague diagnosis paired with a detailed biopsy note is where automated edits start to push back.
Three habits improve claim quality fast:
- Use the most specific documented diagnosis available.
- Link the diagnosis directly to the procedure line.
- Make sure the assessment and procedure note tell the same story.
Medical necessity is a documentation issue first
Coders sometimes treat diagnosis mapping as a front-end claim scrubber task. It's not. It starts in the chart. If the provider documents the symptom, the clinical concern, and the reason for choosing biopsy, the ICD-10 assignment becomes easier and the claim is easier to defend on appeal.
Coding Complex Scenarios Dilation and E/M Services
A claim leaves the office as a routine 58100. Two weeks later it comes back denied because the procedure note mentions cervical dilation, the visit code was billed with modifier 25, and no one stopped to ask whether the encounter was still a simple biopsy. That is how a small coding miss turns into rework, appeal time, and delayed cash.
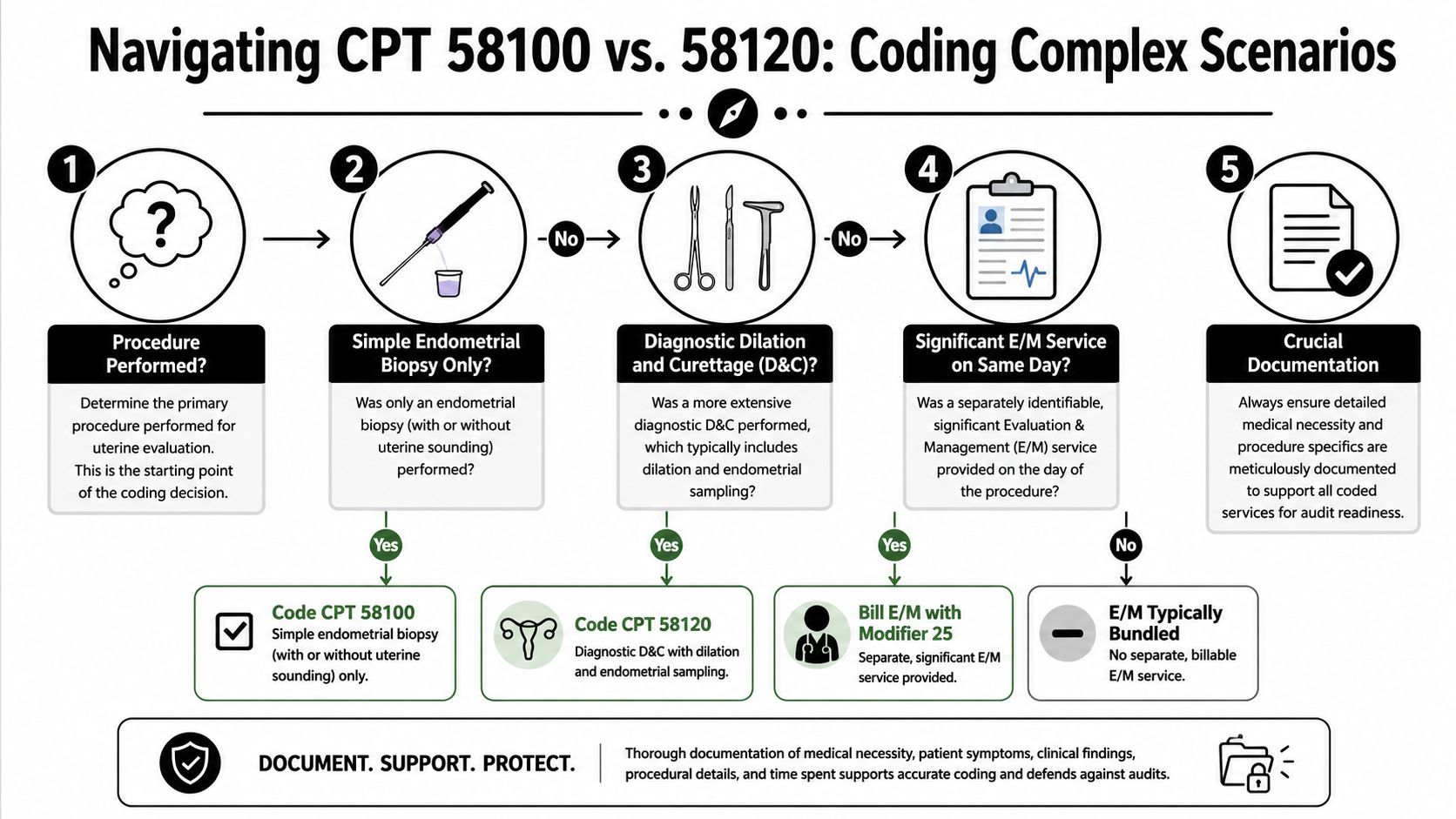
When cervical dilation changes the code
The highest-risk scenario is the note that says the cervix was stenotic, dilation was performed, and endometrial tissue was then obtained. At that point, billing 58100 plus a separate dilation code creates avoidable edit problems. The coding question is no longer whether dilation happened. The question is whether the service crossed into the 58120 pathway.
The Society of Gynecologic Oncology addresses that distinction in its coding note on endometrial biopsy with cervical dilation. For billing teams, the practical rule is simple. Do not code from the scheduling label or the superbill description alone. Code from the operative details.
Use the note to answer four specific questions:
- Was dilation performed, or only attempted?
- Why was dilation needed?
- Was tissue successfully obtained?
- Does the physician describe the service as biopsy, curettage, or both?
Those details decide whether the original code stands, whether 58120 fits better, or whether the claim should be held for clarification.
What I tell new OB-GYN billers to watch for
Certain phrases should stop the claim before it drops:
- “Cervical stenosis” with documented mechanical dilation
- “Dilated cervix to allow passage”
- “Curette used” or “D&C performed”
- “Unable to pass pipelle until dilation performed”
Each phrase changes the coding review. RevGuard's value in this workflow is revenue protection. It catches the claim before the payer does, while the chart is still easy to fix and the provider still remembers what happened.
Same-day E/M services are won or lost in the note
Same-day E/M coding gets overbilled in one direction and underbilled in the other. Some practices append modifier 25 every time an endometrial biopsy happens during an office visit. Others avoid billing the E/M at all because they are tired of denials. Both habits give away revenue or create audit exposure.
The right question is whether the physician documented work beyond the usual pre-procedure assessment. A separate E/M is supportable when the visit includes a real evaluation of a new problem, a review of treatment options, risk discussion, and the decision to proceed with biopsy on that date. It is weak when the note only covers consent, positioning, timeout, and the brief assessment needed to perform the procedure.
A fast chart test helps:
| Documentation pattern | Billing implication | Revenue risk |
|---|---|---|
| New bleeding complaint evaluated, differential assessed, biopsy decision made after workup | E/M may be reported with modifier 25 | Lost revenue if omitted |
| Planned biopsy visit with routine history update and consent | Procedure only in most cases | Denial if E/M is added |
| One blended paragraph for history, decision, and procedure | Hold and query before billing | High denial and appeal burden |
Modifier 25 is defended by separation, not by intention. If the cognitive work is not clearly distinct in the note, the payer will treat it as part of the procedure.
Failed attempts need their own billing logic
Failed biopsy attempts are another denial trap. The provider may document cervical stenosis, patient discomfort, vasovagal symptoms, or inability to pass the instrument. If no tissue is obtained, billing staff cannot clean up the story and submit it as a completed biopsy just because the physician intended to perform one.
That mistake creates two problems. The payer may deny for lack of support, and the record becomes harder to defend if the patient later returns for a successful procedure in the office or operating room.
The chart should answer three points with no guesswork:
- What was attempted
- Why it could not be completed
- Whether any specimen was obtained
If any of those points are missing, stop the claim and query the provider. A short clarification before submission protects revenue better than a long appeal after denial.
Documentation habits that prevent the expensive denials
The strongest notes in these mixed scenarios do not just describe the steps. They explain the turning point. The physician documents that routine pipelle passage was unsuccessful, cervical stenosis required dilation, or the problem-focused visit led to a same-day decision for biopsy after separate evaluation.
That level of specificity matters because these claims often fail for reasons that are avoidable. The payer sees 58100, reads “dilated cervix” in the note, and downcodes or denies. The payer sees an E/M with modifier 25, but the chart reads like a standard pre-procedure visit, and the E/M is cut. The payer sees a completed procedure code, but the note says the biopsy was attempted and aborted.
Those are not abstract coding issues. They are front-end revenue leaks. The fix is disciplined documentation, claim holds for ambiguous charts, and appeal language tied to the actual sequence of care.
Navigating Common Denials and Payer Edits
The claim leaves clean. Ten days later it comes back denied because the payer read the note differently than your team did. That is the pattern with endometrial biopsy CPT claims. The procedure itself is straightforward. The denials usually come from what surrounded it: why it was done, whether it was completed, whether cervical work changed the coding path, and whether a same-day E/M was justified as separate.
Four denial categories account for most of the avoidable rework.
Denial category one medical necessity edits
These denials start when the diagnosis on the claim does not match the documented indication for the biopsy. I see this most often when the assessment lists several gynecologic problems, but the coder links a general symptom instead of the condition that led to the decision to sample the endometrium.
The fix is a line-level review before release. The indication in the procedure note, the assessment, and the ICD-10 linkage all need to point to the same clinical reason. If they do not, hold the claim and correct it before filing. That one front-end stop protects revenue better than a routine appeal queue.
Watch repeat claims closely. If a first attempt failed and the patient returns later for a completed biopsy, the diagnosis may still be appropriate, but the documentation has to show why the later encounter was medically necessary and distinct from the earlier visit.
Denial category two procedure-status confusion
Payers deny these claims when the chart does not make clear whether the biopsy was completed, partially completed, or attempted but abandoned. That confusion gets expensive fast. A submitted 58100 with a note that says "unable to pass pipelle" is an open invitation for denial, recoupment, or both.
Audit for these questions before claim submission:
- Was endometrial tissue obtained?
- Did the physician document the method used?
- Did the note describe a failed attempt instead of a completed biopsy?
- Was cervical stenosis or dilation documented in a way that changes how the payer may edit the claim?
This is one of the unwritten rules in gynecology coding. The payer is not reading for clinical nuance. The payer is looking for mismatch. If the claim says completed biopsy and the note reads like an aborted attempt, the payer wins the first round.
Denial category three bundling and incidental service edits
Bundling denials usually show up in the what-if cases. The physician performs the biopsy, documents difficult cervical access, and the bill drops with extra procedural lines that the payer treats as incidental or included. Some edits are correct. Some are lazy payer processing. Your team needs to know the difference before filing an appeal.
Start with the operative note and ask one practical question: was there a distinct, separately reportable service, or was this just the work required to get the biopsy done? If the extra work was inherent to completing the procedure, the denial may stand. If the documentation supports a separate service with its own medical reason and work, then appeal with that sequence laid out clearly.
A weak appeal argues code definitions in the abstract. A strong appeal explains exactly what happened during the encounter and why the denied service was not part of the usual biopsy package.
Denial category four modifier edits, especially modifier 25
Same-day E/M denials are rarely about whether the physician saw the patient. They are about whether the record supports a significant, separately identifiable evaluation beyond the usual pre-procedure work.
Modifier 25 should survive review only when the note shows a real evaluation that changed management or established the need for the biopsy after separate assessment. If the documentation reads like routine consent, history confirmation, and procedure prep, expect the E/M to be cut.
Train billers to test the note against three questions:
- Did the physician evaluate a problem beyond the work normally done before the biopsy?
- Did that evaluation lead to medical decision-making that stands on its own?
- Can an auditor find that separate work without guessing?
If the answer is unclear, do not bill on optimism. Query first. RevGuard's value in this workflow is revenue protection through discipline. Stop weak modifier claims before they create denials that cost more to fight than they are worth.
How to work denied claims without wasting appeal labor
Not every denial deserves an appeal. Triage them.
Appeal when the documentation supports a completed biopsy, a properly linked diagnosis, or a separate E/M that the payer ignored. Correct and rebill when the claim was filed with the wrong diagnosis linkage, the wrong modifier decision, or a note that never supported the billed service in the first place.
For high-friction payers, build denial templates around the scenarios that recur:
- completed biopsy misread as failed attempt
- cervical stenosis documented, but payer treated the claim as improperly unbundled
- modifier 25 denied despite separate problem evaluation
- diagnosis linked incorrectly at the line level
That is how experienced RCM teams reduce preventable write-offs. They do not just post denials. They sort payer behavior, tighten documentation rules, and keep the same weak claim from leaving the office twice.
Reimbursement Ranges and Expectations for 2026
The reimbursement question comes up early, but it should come after coding accuracy. A claim paid at the wrong rate because it was miscoded or under-supported isn't a successful outcome. It's a delayed denial risk.
For 2026, think about payment for endometrial biopsy through the lens of the fee schedule structure and contract terms, not as one universal number. Reimbursement varies by payer, geography, and site of service. Medicare methodology relies on RVU-based payment logic, and commercial contracts may map differently depending on how the plan applies office procedure rates.
What billing teams should actually track
Instead of chasing a generic benchmark, monitor these operational signals:
- Expected allowed amount by payer and place of service: Your contract matrix should tell you what the claim should pay if processed correctly.
- Variance between submitted and paid code sets: Underpayments often start with a subtle payer reclassification.
- Denial-to-payment cycle time: A procedure that should pay cleanly loses value when staff must touch it multiple times.
- Global period awareness: Follow-up billing should be reviewed against package rules before claim release.
If your team needs a cleaner framework for understanding how payers classify and route charges, this explanation of revenue codes in healthcare billing is useful context.
The real benchmark
The benchmark isn't a dollar figure printed on a cheat sheet. The benchmark is whether your practice consistently receives the payment your documentation, coding, and contract support.
For 58100, that means the reimbursement conversation should always begin with one question. Did we submit the exact service that the chart proves?
Appeal and IDR Strategies for Underpayments
A payer trims payment on a clean 58100 claim, or denies it outright, and the remittance reason points your team in the wrong direction. New billers often start with the ERA. I train them to start with the chart, the submitted code set, and the contract.

Build the appeal around the exact failure point
Underpayment work on endometrial biopsy claims gets sloppy when staff argue the whole case instead of the specific issue the payer acted on. Separate these first:
- Medical necessity denial: Match the indication in the assessment and plan to the diagnosis billed.
- Procedure mismatch: Confirm whether the chart supports 58100, a different procedure, or a failed attempt that was never completed.
- Bundling or modifier edit: Check whether the payer reduced payment because of an E/M service, another procedure, or a modifier they consider unsupported.
- Pure underpayment: Compare the paid amount to your contracted expected allowance for the code, modifier, and place of service.
That distinction matters because appeals fail for different reasons. If the physician documented cervical stenosis, attempted biopsy, then performed dilation to complete a more extensive service, the recovery path may be a corrected claim, not an appeal defending the original code. If the chart supports a separate problem-oriented E/M with modifier 25, the appeal should quote the note elements that show decision-making beyond the procedure itself.
What belongs in the packet
A useful appeal packet is short, chart-based, and specific. Include only the pages that prove your point:
- Procedure note showing what was attempted and what was completed
- Assessment and plan establishing the reason for sampling
- Diagnosis linkage that matches the documented indication
- Original claim form and remittance so the reviewer can see exactly how the payer processed it
- Contract excerpt or expected reimbursement reference if the dispute is underpayment rather than medical necessity
- Concise appeal letter that states the requested action in one sentence
I also want one line in the letter that answers the payer's likely objection before they raise it. If the denial turns on cervical dilation, say whether dilation was incidental, whether the biopsy was completed, and whether the submitted CPT code was meant to represent only the sampling or the full service documented. If the dispute involves a failed attempt, say that clearly. Payers often deny these claims because the note reads like an intended procedure, not a completed one.
When to appeal, when to correct, when to stop
Revenue protection depends on choosing the right route early.
| Situation | Best next step |
|---|---|
| 58100 was performed, documented clearly, and denied despite correct diagnosis linkage | Appeal |
| Claim was billed as 58100, but the chart supports a different procedure after dilation | Correct and resubmit if timely filing allows |
| Modifier 25 was appended, but the note only covers the usual pre-procedure work | Stop the appeal and educate the provider |
| Paid amount falls below contract terms with no coding issue | Appeal as underpayment |
| Procedure was attempted but not completed, and documentation does not support the submitted code | Correct, void, or write off based on payer rules |
This is the unwritten rule. A weak appeal burns staff time twice. You lose the first appeal, then someone has to reopen the chart and fix a coding issue that should have been identified on day one.
IDR is not the first tool
Independent Dispute Resolution has a place, but only after your team has exhausted the ordinary recovery path and confirmed the dispute is really about final payment, not coding accuracy or missing documentation. If the claim failed because the note never established a separately identifiable E/M service, IDR will not rescue it. If the payer acknowledged the service and still paid below the applicable amount after the required dispute steps, escalation makes more sense.
Teams that handle repeated OB-GYN underpayments well usually formalize these decisions in a workflow, not in individual inboxes. A disciplined healthcare denial management process helps staff sort coding corrections from collectible underpayments before appeal deadlines expire.
The practical standard is simple. Every 58100 claim should be appeal-ready before it leaves the office. That means the chart can answer three questions without guesswork: why the biopsy was medically necessary, what was performed, and why the submitted code set matches that record.
If your practice is seeing avoidable denials, underpayments, or repeated rework on gynecology claims, RevGuard helps provider organizations protect revenue across the full claim lifecycle, from coding and denial prevention to payment recovery and dispute escalation.