Monday starts with a denial workqueue that looks manageable. By Wednesday, your team is buried in rejections from multiple payers, each with its own edits, enrollment quirks, and response files. One claim is missing a subscriber detail. Another has a diagnosis and procedure mismatch. A third never reached the payer because it was routed incorrectly. None of these problems are catastrophic on their own. Together, they slow cash, frustrate staff, and turn billing into a daily cleanup project.
That's where many specialty practices get stuck. They assume the main battle starts after a payer adjudicates the claim. In practice, the trouble usually starts earlier, before the claim ever gets there. If the front end is messy, every downstream step gets more expensive. Coders rework charts. Billers resubmit. Managers chase status updates. Providers wonder why volume looks strong while collections lag.
A clearinghouse in medical billing fixes that bottleneck when it's set up and used correctly. Not because it's magic, and not because it eliminates all denials. It works because it standardizes, validates, and routes claims before payer systems can reject them for avoidable reasons. For specialty groups dealing with complex coding, out-of-network exposure, or No Surprises Act disputes, that front-end discipline does more than improve workflow. It protects revenue.
The Hidden Bottleneck in Your Revenue Cycle
The practice manager usually sees the symptom first. Days in A/R feel heavier. Staff spend more time reading rejection reports than posting payments. Payer portals become a second full-time job. Meanwhile, the physicians hear a simpler summary: “We're waiting on insurance.”
That answer obscures the primary problem. Many practices don't have a payer problem first. They have a claim quality problem first.
Where the backlog actually starts
A claim leaves the practice management system with a small defect. Maybe the insurance ID is off by one character. Maybe the rendering provider record doesn't match payer enrollment. Maybe the coding is sound, but the format doesn't line up with what that payer accepts. If the claim goes straight out without a strong checkpoint, the billing office learns about the error late, after time has already been lost.
For specialties, this compounds quickly. Anesthesia, orthopedics, radiology, gastroenterology, and air ambulance claims often involve tighter documentation, more coding nuance, and more payer scrutiny. A weak submission process creates friction at scale.
Practical rule: Every preventable rejection should be treated as a process defect, not just a claim defect.
Why teams feel overloaded
When claim traffic is fragmented across payer portals, manual edits, and disconnected reports, staff can't see the full picture. They work reactively. They fix what bounced back today, then hope tomorrow's batch behaves better.
A clearinghouse changes that operating model. It becomes the central checkpoint between your billing system and the payer network. Instead of letting each payer expose errors in its own way, the clearinghouse catches many of them earlier, where corrections are faster and cheaper.
That's the hidden advantage. Better claims in. Cleaner adjudication flow out. Less rework in the middle.
What Exactly Is a Medical Billing Clearinghouse
A medical billing clearinghouse is the digital translator and delivery hub between your practice and insurers. If your billing system creates the claim, the clearinghouse makes sure that claim is in the right format, passes basic and payer-specific edits, and reaches the correct destination.
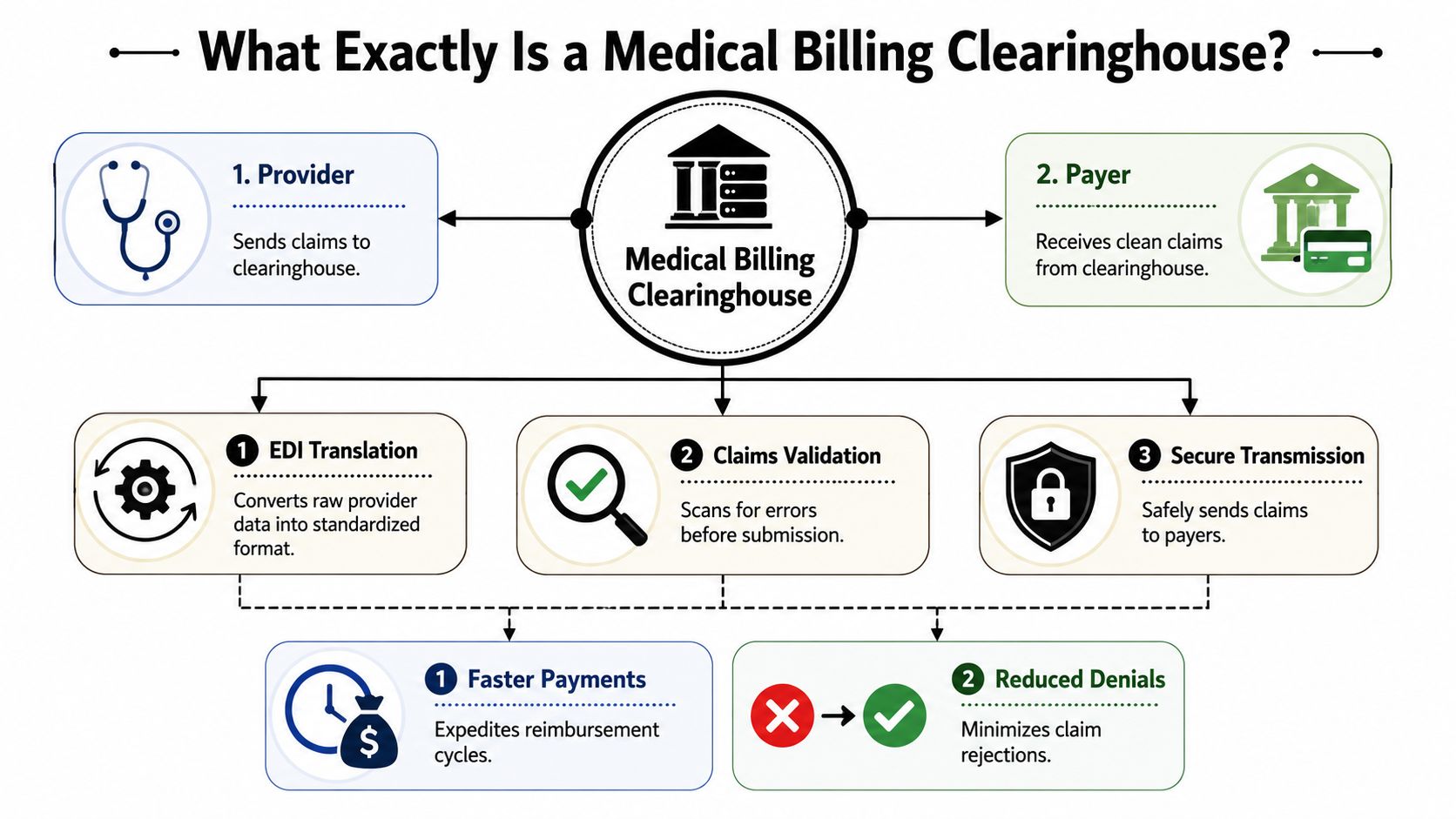
Think of it as a translator and post office
The post office analogy works because a clearinghouse handles both preparation and delivery. Your team creates the “letter,” but the clearinghouse checks whether the address is usable, whether the contents meet the destination's rules, and whether the message needs to be converted before it can be accepted.
That translation role isn't just a convenience. Under HIPAA, a clearinghouse has a defined function in the transaction ecosystem. HRSA explains that a clearinghouse can translate between standard and non-standard healthcare transaction formats, including converting provider data into the HIPAA 837 claim format required for submission and payment, and notes that this role can expedite turnaround from claim submission to payment, as outlined in HRSA's clearinghouse definition.
Why this matters operationally
Without a clearinghouse, a provider would need to account for each payer's formatting expectations and connection path far more directly. That creates extra manual work, more brittle interfaces, and more chances for claims to fail before they're even reviewed for payment.
In a functioning revenue cycle, the clearinghouse usually sits in the middle of these activities:
- Claim intake from the practice system so billers aren't building separate workflows for every payer
- Data translation into HIPAA-standard transactions so the claim can move electronically through payer channels
- Validation before transmission so basic defects don't become payer-facing failures
- Response handling on the return path so status, remittance, and error information can get back into billing operations
What a clearinghouse is not
It isn't the payer. It doesn't decide medical necessity, payment amount, contract interpretation, or final denial outcome. It also isn't a replacement for clean registration, strong coding, or payer enrollment discipline.
A clearinghouse is infrastructure. When practices treat it like a simple mailroom, they miss most of its value.
The right way to view it is as a control point. It's where formatting, validation, and routing happen before payer adjudication starts. For a specialty practice manager, that makes it one of the few tools that affects both staff workload and cash flow at the same time.
The Three Core Functions That Drive Clean Claims
A good clearinghouse earns its keep in three places: translation, scrubbing, and routing. If any one of those is weak, claims either fail early or create unnecessary work later.

Translation turns practice data into payer-ready transactions
Your PM or EHR doesn't naturally speak every payer's preferred transaction language. The clearinghouse converts provider-generated data into the standardized electronic structure needed for submission. That keeps your team from building custom connections across a fragmented payer mix.
This matters most when your specialty has multiple sites, hospital-based billing, or mixed commercial and government business. The more payer variation you have, the more valuable that standardization layer becomes.
Scrubbing catches mistakes while they're still cheap
This is the highest-value function operationally. Trubridge describes claim scrubbing as the use of deterministic validation rules to detect missing data, invalid modifiers, duplicate submissions, and mismatched patient or payer identifiers before transmission, and notes that clean-claim workflows reduce manual follow-up while clearinghouse responses support denial tracking and payment posting through clearinghouse claim scrubbing and response workflows.
That sentence sounds technical. The practical meaning is simple. It's cheaper to fix a bad claim before it leaves your system than after it bounces back from a payer.
Common front-end catches include:
- Registration defects like wrong subscriber details or missing patient fields
- Coding edits such as invalid modifiers or diagnosis-procedure mismatches
- Duplicate claim flags that prevent unnecessary resubmissions
- Payer identifier issues that stop claims from going to the wrong destination
Eligibility work supports this front-end discipline too. If your team wants fewer claims to fail for coverage-related reasons, tightening medical eligibility verification workflows upstream usually pays off.
Routing determines whether a clean claim actually lands correctly
A claim can be accurate and still fail operationally if it's sent down the wrong channel. Intelligent routing maps the claim to the correct payer endpoint and transaction path. That sounds basic until you manage carve-outs, delegated arrangements, or payers with multiple submission rules across product lines.
What works and what doesn't
What works is a clearinghouse configuration that reflects your actual payer mix and specialty billing reality. What doesn't work is turning on default edits and assuming the setup is finished.
If the rejection report keeps surfacing the same issue, the answer usually isn't “work harder.” It's “change the edit, fix the source data, or both.”
Practices get the most value when they review recurring rejection patterns with billing, coding, and registration together. Clean claims aren't created by one department. They're built by a connected process.
How a Clearinghouse Fits into the Claims Lifecycle
A clearinghouse only makes sense when you place it inside the full revenue cycle. It isn't a side tool. It's the checkpoint between claim creation and payer adjudication, and it also helps carry payer responses back into your workflow.
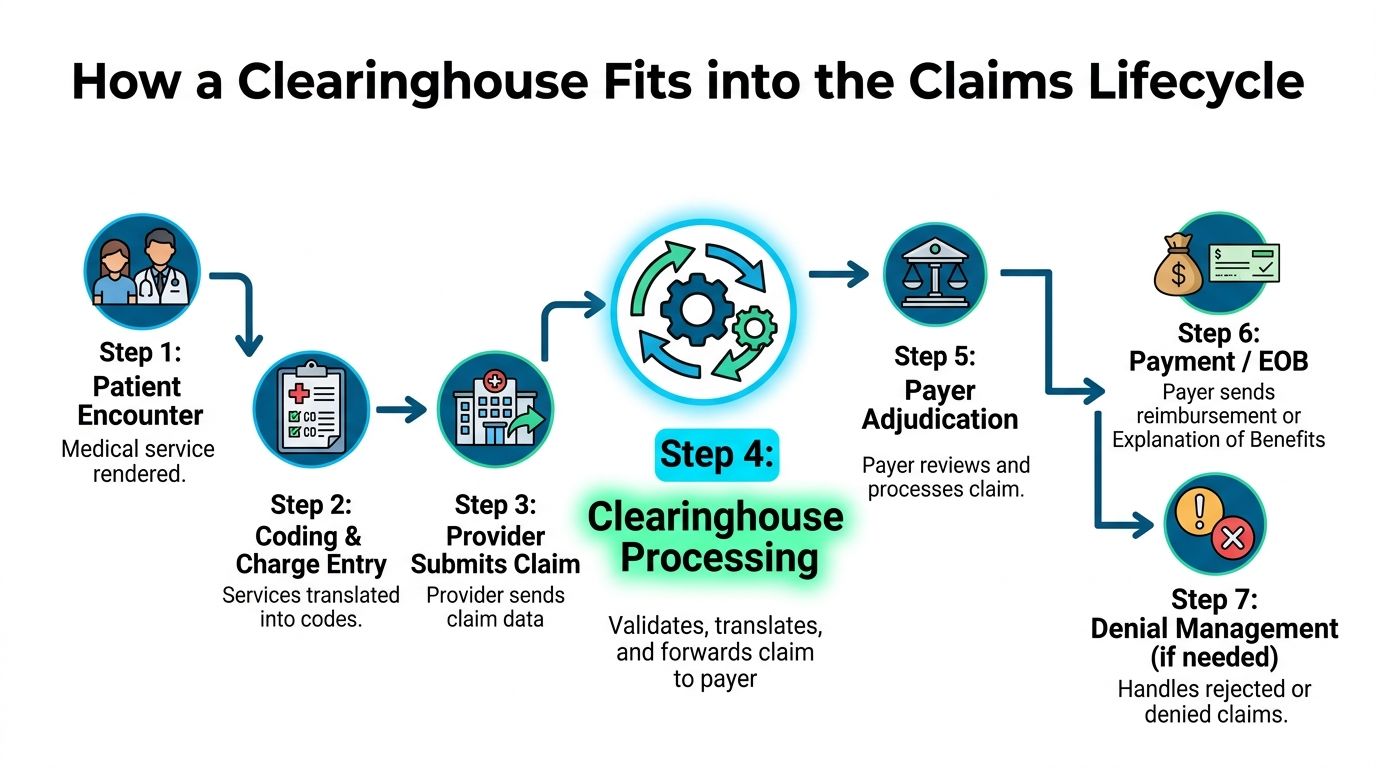
The clearinghouse sits in the middle, not at the edge
Here's how the process works: A patient encounter happens. Charges are entered. Coding is assigned. The provider system generates the claim. Then the clearinghouse validates, translates, and routes it before the payer reviews it. After adjudication, the response comes back through remittance and claim-status transactions so the billing team can post payment, identify denials, or work exceptions.
That middle position is why a clearinghouse has such broad impact. It influences what leaves your system and what comes back into it.
What moves through this checkpoint
In modern workflows, the clearinghouse does more than pass claims along. Industry descriptions include claim scrubbing, payer routing, eligibility verification, and remittance advice delivery, and some vendors report benchmarks such as 98% first-pass claim rates and 40% fewer denials as examples of the performance clearinghouse-enabled claims processing can support in revenue cycle management, according to this overview of clearinghouse workflow and metrics.
That kind of benchmark matters less as a promise and more as a direction. The point isn't that every practice will hit the same figures. The point is that better front-end controls can materially change claim quality and denial pressure.
Why downstream teams care
When the clearinghouse is working properly, several things happen at once:
- Billers get faster feedback on whether claims were accepted, rejected, or need correction
- Posting teams receive cleaner remittance flow instead of chasing scattered files
- Managers can track bottlenecks by stage rather than guessing where cash is stalling
- Denial teams can distinguish pre-adjudication failures from payer decisions and assign work correctly
If your team is also trying to tighten follow-up after payer review, understanding the claim adjudication process helps separate submission problems from actual payment disputes.
The lifecycle view changes decision-making
Practices often buy a clearinghouse based on transaction convenience. The smarter approach is to judge it by lifecycle visibility. Can your staff see where claims are stuck? Can they tell whether failures start in registration, coding, enrollment, routing, or payer response? Can they standardize workqueues from ERA and claim-status files instead of handling every exception manually?
Those questions matter because payment delay rarely comes from one dramatic failure. It usually comes from hundreds of small handoff problems across the claim lifecycle.
Selecting the Right Clearinghouse for Your Specialty Practice
A specialty practice shouldn't shop for a clearinghouse the way a general primary care office might. Your claims are often more complex, your payer friction is higher, and the cost of avoidable errors is heavier. The right choice is less about feature count and more about operational fit.
The wrong fit usually shows up in three places
First, the payer footprint looks broad on paper but misses the plans that matter most to your group. Second, the edits are generic and don't reflect specialty billing patterns. Third, staff can't get actionable reporting without exporting data into spreadsheets and rebuilding the story by hand.
Those gaps don't just annoy the billing office. They affect cash forecasting, denial prevention, and dispute readiness.
What to evaluate before you sign
| Evaluation Criteria | What to Look For | Why It Matters for a Specialty Practice |
|---|---|---|
| Payer connectivity | Strong coverage across your highest-volume commercial, government, and regional payers | Specialty groups often have concentrated payer exposure, so missing one major connection creates workflow drag fast |
| Specialty-specific edits | Rules that reflect your coding, modifier use, and documentation patterns | Generic edits miss specialty failure points and create false confidence |
| PM and EHR integration | Stable data flow with your current systems and clear error reporting | If staff has to rekey or manually reconcile files, rejection risk climbs |
| Reporting visibility | Dashboards for rejections, acceptance trends, payer response flow, and remittance status | Managers need to identify where claims are failing, not just that they failed |
| Enrollment support | Structured onboarding for payer enrollment and ongoing maintenance | A technically strong clearinghouse still stalls if payer enrollment is incomplete |
| ERA and status handling | Clean return files and usable status updates inside the billing workflow | Back-end efficiency matters almost as much as submission quality |
| Support model | Teams that understand billing operations, not just ticket triage | Specialty practices need issue resolution that connects technical errors to revenue impact |
| Scalability | Ability to support multiple locations, TINs, NPIs, and growth | Expansion breaks weak configurations quickly |
Questions worth pressing vendors on
Ask them how they handle payer-specific edits that differ by product line. Ask what happens when a claim is rejected at the clearinghouse versus accepted there and later denied by the payer. Ask how enrollment delays are surfaced. Ask whether reporting shows root causes or just message dumps.
If you're comparing broader RCM support models, this is also where some practices look at vendors that connect front-end claim quality to downstream revenue protection. For example, RevGuard works across specialty RCM and IDR workflows, which is relevant when a practice wants cleaner, dispute-ready claims rather than a transmission tool alone.
Don't choose a clearinghouse based only on who can submit a file. Choose based on who helps your team prevent avoidable rework.
What usually works best
For most specialty groups, the winning setup includes strong payer routing, transparent rejection reporting, dependable integration with the current PM system, and support staff who can talk through both transaction errors and operational consequences. A cheaper option often becomes expensive if your billing team spends hours translating cryptic edits into manual fixes.
Troubleshooting Common Clearinghouse Issues
Even good clearinghouse setups break in predictable ways. The key is knowing whether the problem started before submission, during transmission, or after payer receipt. That distinction keeps staff from chasing the wrong fix.
Rejections and denials are not the same problem
A clearinghouse rejection means the claim failed before it reached payer adjudication. A payer denial means the payer received the claim and made a negative payment decision or processing determination. Staff should route those issues differently.
Use this quick rule set:
- If the clearinghouse rejected it, check formatting, demographic fields, payer IDs, provider identifiers, and edit messages first
- If the payer denied it, review coverage, coding support, medical necessity, authorization, contract logic, and documentation
- If you can't tell which happened, verify whether there's payer acceptance confirmation before assigning follow-up work
Enrollment issues can stop clean claims cold
A surprisingly common problem has nothing to do with coding. The claim is technically fine, but the payer enrollment or electronic setup isn't complete for the billing provider, rendering provider, or remit path.
When that happens, staff should verify:
- Provider enrollment status for the payer and line of business
- Correct identifiers on the claim and in the clearinghouse profile
- ERA enrollment alignment if payment files aren't returning properly
- Recent credentialing or ownership changes that may have disrupted existing setup
A clean claim still won't move if enrollment and identity records don't match across systems.
Integration failures need a source-of-truth check
When claim data looks wrong in the clearinghouse, don't start by blaming the clearinghouse. Pull the original claim data from the PM or EHR. Compare key fields. Then determine whether the error was created in source data, in the export mapping, or during clearinghouse validation.
Teams solve these issues faster when they assign one source of truth for each field. Registration owns demographics. Coding owns claim content. Credentialing owns provider records. IT or the vendor manages interface mapping. Without that clarity, the same problem keeps resurfacing under different ticket numbers.
Beyond Submission Advanced RCM and IDR Readiness
A clearinghouse's value isn't limited to getting claims out the door. In specialty reimbursement, especially where out-of-network payment disputes and No Surprises Act pressure exist, the clearinghouse helps create the documented claim trail that supports revenue defense later.
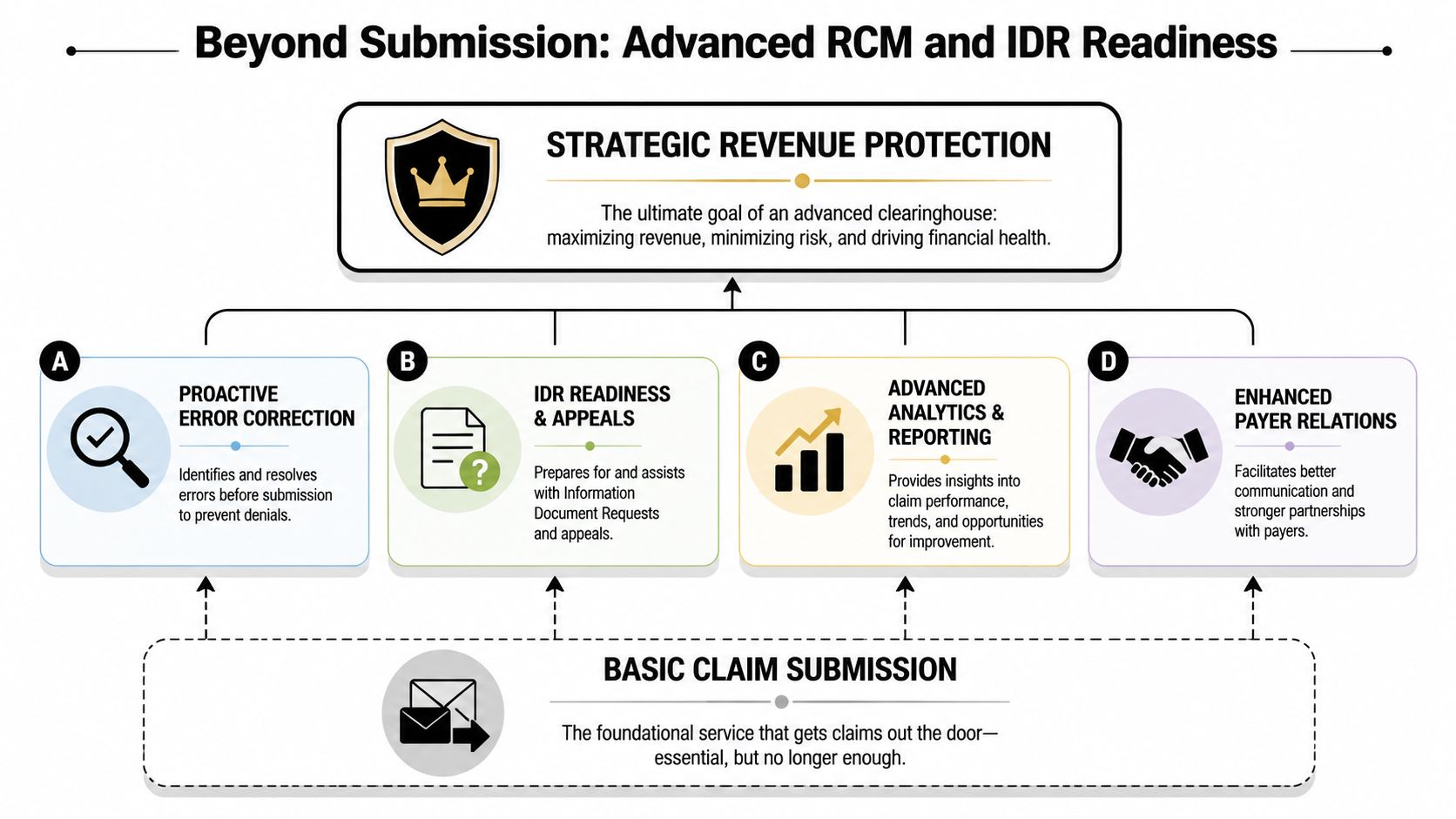
Clean claims create stronger dispute records
A clearinghouse converts provider-generated data into standard X12 transactions, commonly including 837 for claim submission, 270/271 for eligibility, 276/277 for claim status, and 835 for electronic remittance advice, allowing one provider system to communicate with many payer endpoints without custom insurer-by-insurer integrations. HIPAAT Journal also notes that by normalizing nonstandard fields and checking payer-specific edits, the clearinghouse reduces format-related rejections before adjudication and shifts failure points back to the provider side where they are cheaper to correct, as described in this explanation of clearinghouse transaction roles and reimbursement impact.
That matters for more than reimbursement speed. It creates a cleaner chronology of submission, acceptance, status movement, and payment response.
Why this matters for IDR and appeals
Independent Dispute Resolution is evidence-heavy. If a payer underpays, delays, or contests the claim, your position is stronger when the underlying claim history is organized, clean, and traceable. A sloppy submission record weakens the dispute before the argument even starts.
For specialty practices, the first step in a dispute-ready claim isn't writing the appeal letter. It's generating a claim that survives front-end validation, carries the right identifiers, and produces a usable transaction record from submission through remittance.
That's one reason denial prevention and dispute preparation should be linked. If your team is building stronger upstream controls, it also helps to tighten healthcare denial management workflows so payer patterns are visible earlier and appealed more consistently.
The strategic shift
A mature revenue cycle treats the clearinghouse as part of revenue protection, not just transaction transport. It supports cleaner claims, cleaner payment data, and cleaner evidence when reimbursement disputes escalate. For managers in high-complexity specialties, that's the shift that matters most. Better clearinghouse discipline doesn't just reduce administrative headaches. It improves your ability to defend the value of care when a payer challenges payment.
If your specialty practice is trying to reduce avoidable denials, tighten claim quality, and build dispute-ready workflows under the No Surprises Act, RevGuard provides specialty-focused RCM and IDR support across the revenue lifecycle. It's built for provider groups that need cleaner submissions upstream and stronger enforcement when payers underpay downstream.