
Payers do not need to deny a claim to reduce its value. They can approve it at the wrong rate, reprice it through payer-specific logic, downcode it, or apply contract terms the practice does not challenge. For specialty groups and ASCs, that is often where the larger revenue leak sits.
That changes how a CFO should assess medical billing companies in 2026. Clean-claim rates and denial follow-up still matter, but they do not answer the harder question: who is finding adjudicated dollars that never reached expected reimbursement, and what happens when recovery requires formal dispute work under the No Surprises Act?
A disciplined vendor review starts with the post-claim operating model. The right partner can trace variance between expected and paid amounts, isolate payer patterns by CPT, location, and contract terms, and route the right cases into appeals, reconsiderations, or IDR. Practices that want that level of control usually need a billing partner with a defined revenue cycle optimization strategy for underpayment recovery and payer variance analysis, not a vendor built only to move claims through clearinghouse edits.
The distinction is operational, not cosmetic.
| Evaluation lens | Basic billing vendor | Revenue protection partner |
|---|---|---|
| Core objective | Submit claims and post payments | Defend full collectible reimbursement |
| Primary KPI | Clean claims or submission volume | Net collection quality, A/R discipline, underpayment recovery |
| Specialty handling | General workflows | Specialty-specific payer and coding logic |
| Denial response | Rework after rejection | Prevent, analyze root cause, and escalate when needed |
| Underpayment strategy | Often limited or unclear | Structured recovery and dispute readiness |
| CFO visibility | Periodic reports | Actionable dashboards and payer-behavior insight |
| NSA and IDR readiness | Rarely central | Built into operating model for affected specialties |
For high-acuity and out-of-network exposed specialties, IDR capability is not a niche feature. It is part of revenue defense. A billing company that cannot document payment variance, support open negotiation, and manage IDR timelines may post cash efficiently while still leaving meaningful reimbursement behind.
The High Cost of Inefficient Medical Billing
Payment variance is often a larger financial risk than the claims that never pay at all. For specialty practices and ASCs, the expensive failure is rarely a single rejected claim. It is the steady acceptance of payer behavior that erodes reimbursement after adjudication through downcoding, partial payment, missed carve-outs, and unresolved out-of-network disputes.
That distinction changes how a CFO should evaluate medical billing companies. A vendor can keep charge entry moving and maintain acceptable denial metrics while still allowing meaningful post-claim leakage. In procedural and high-acuity specialties, that leakage shows up in small line-item reductions, delayed follow-up on short pays, and missed escalation windows that permanently limit recovery.
Why CFOs should treat billing as a strategic function
A low-fee billing arrangement can become expensive in ways the invoice never captures. If the team posts payments without testing them against contract terms, usual reimbursement patterns, or NSA-related dispute opportunities, the practice gives up margin. The loss does not appear as a dramatic operational failure. It appears as lower yield per case, weaker payer accountability, and less credible data in future contract discussions.
Practical rule: If your billing partner cannot explain where reimbursement falls short after adjudication, they are processing claims rather than protecting revenue.
A stronger evaluation standard looks beyond staffing ratios and collection slogans. Finance leaders need to know whether the billing company can identify underpayment trends by payer, service line, and site of care, then route each variance into the right recovery path. For many groups, that starts with a defined revenue cycle optimization strategy for underpayment recovery and payer variance analysis, not a narrow outsourcing decision based on submission volume.
The hidden cost of “good enough”
Operationally, mediocre billing often looks busy enough to pass. Claims go out. Payments come in. Aging stays within a tolerable range. Yet the practice remains structurally under-collected because no one is measuring expected reimbursement against actual reimbursement with enough precision to challenge payer behavior.
The downstream effect is larger than monthly cash. Chronic underpayment tolerance weakens forecasting, distorts physician productivity economics, and limits a group's ability to decide which contracts, service lines, or facilities are performing. In specialties exposed to out-of-network claims or NSA dispute workflows, the cost rises again. Missing open negotiation deadlines or failing to assemble a supportable IDR file can turn a recoverable balance into a permanent concession.
Inefficient billing, then, is not just an administrative drag. It is a revenue defense problem.
Beyond Clean Claims The New RCM Mandate
A clean claim rate still matters. It just doesn't tell you enough.
Many medical billing companies market around first-pass performance because it's easy to understand and easy to promote. But a claim can be technically clean at submission and still produce a poor financial outcome later. Payers can deny, downcode, partially reimburse, or approve at a level that doesn't reflect the contract, documentation, or out-of-network protection pathways available to the provider.
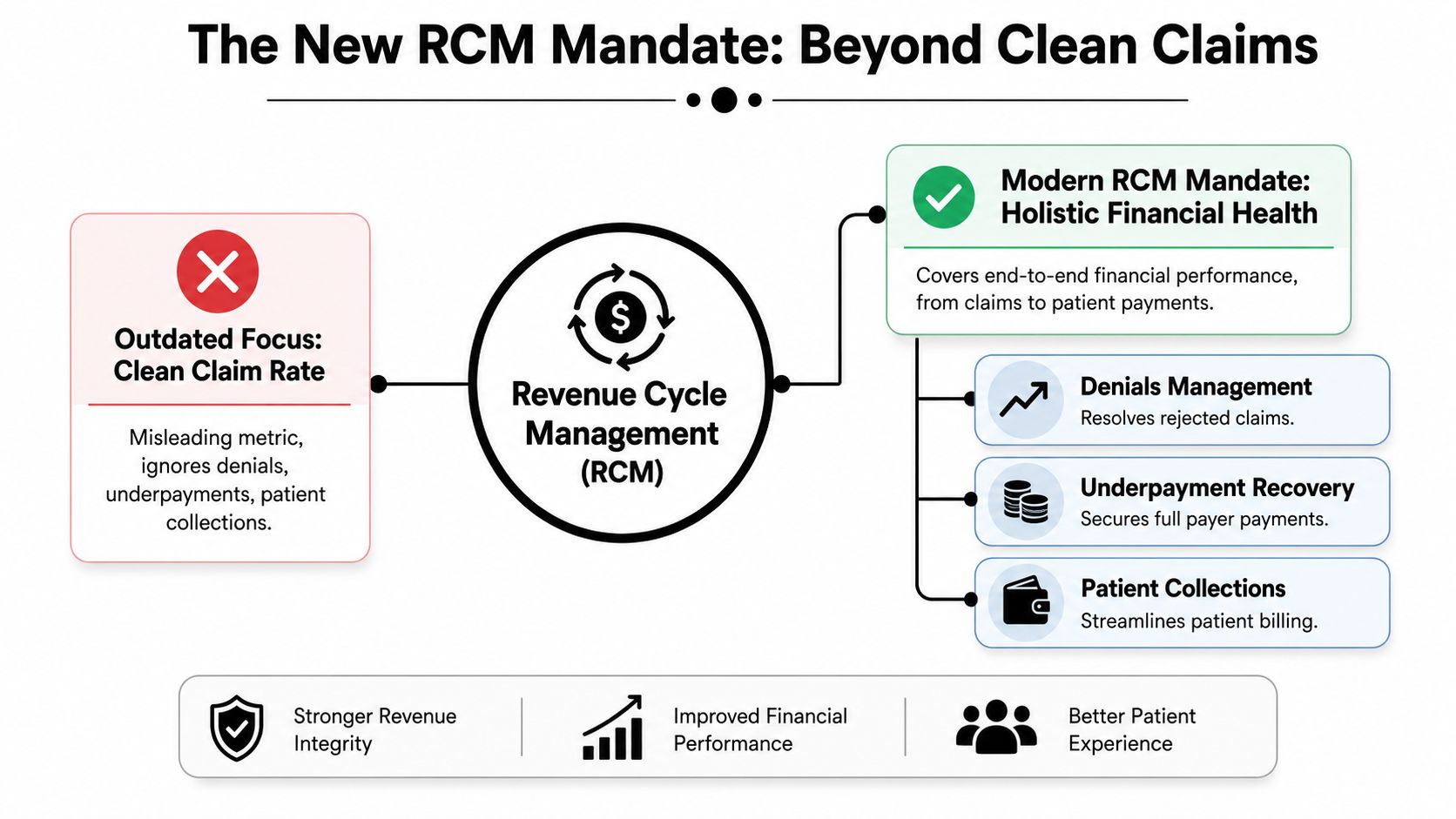
Why clean claim thinking breaks down
The modern revenue problem is partly visible and partly hidden. While 10-15% of claims are officially denied, the hidden loss from underpayments is often larger, and this gap is missed by 90% of current market coverage on billing companies, according to Human Medical Billing's discussion of what generic guides miss. That matters because a denial gets attention. An underpayment often gets posted, tolerated, and forgotten.
Many billing relationships fail specialty groups. They build workflows around rejection management but not reimbursement enforcement. They can refile and appeal, but they can't trace payer behavior patterns across procedure sets, identify systematic downcoding, or convert approved-but-underpaid claims into recoverable revenue.
The post-claim battlefield
The old RCM model assumed the claim was the event. The current payer environment treats adjudication as the midpoint. After submission, the actual work may include:
- Payment variance review: Compare paid amounts against contract terms, expected reimbursement logic, and specialty-specific patterns.
- Downcoding detection: Identify when the payer changes the code logic or service intensity in ways that reduce reimbursement.
- Dispute readiness: Preserve documentation, timelines, and evidence that support a later challenge.
- Arbitration strategy: In applicable scenarios, move beyond standard appeals into formal dispute mechanisms.
The organizations with the strongest reimbursement outcomes don't stop at claim acceptance. They engineer claims to be defensible after payment.
Why IDR now belongs in vendor evaluation
For affected specialties, the No Surprises Act changed what a serious billing partner must be able to do. A vendor may still be competent at eligibility, coding, charge entry, and denials, yet remain financially incomplete if it has no Independent Dispute Resolution (IDR) capability or no operating connection between RCM and IDR.
That link is critical because the best arbitration files are usually built upstream. Documentation quality, coding precision, payer-specific context, and timeline control all shape whether a disputed reimbursement can successfully be defended. Firms that treat IDR as a separate legal afterthought usually lose the operational advantage before the dispute starts.
If you're assessing modern medical billing companies for complex specialties, include the question of how RCM and IDR work together inside one coordinated workflow. If the answer is vague, the vendor is probably still selling yesterday's model.
The 7-Point Vendor Evaluation Framework
A vendor that raises collections by one or two points can change specialty-practice economics more than a high clean-claim rate ever will. The reason is simple. The largest losses often occur after the claim is accepted, when payers reprice, downcode, delay, or underpay in ways that are easy to post and easy to miss.
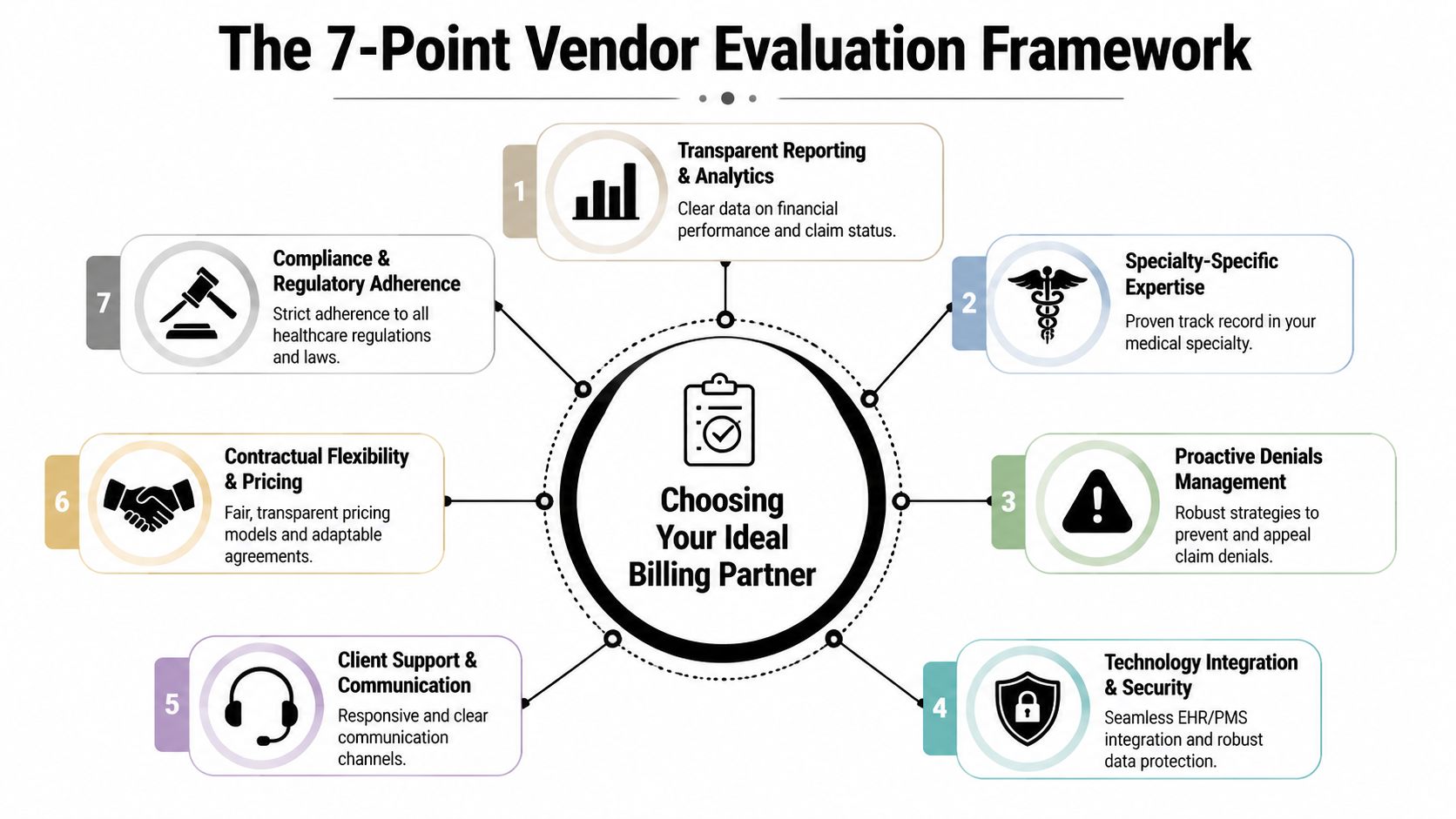
A useful evaluation framework measures whether a billing partner can protect expected reimbursement across the full payment cycle. That means specialty fluency, disciplined follow-up, and a documented process for challenging payer behavior after adjudication. For groups comparing outsourced revenue cycle management for specialty practices, the goal is not activity volume. The goal is retained revenue.
1. Specialty-specific operating depth
Specialty complexity shows up in workflow design, not in marketing claims. Air ambulance, anesthesia, GI, orthopedics, and dermatology each create different authorization risks, coding dependencies, payer edits, and reimbursement disputes.
P3 Care's review of generic billing comparisons points out how little many vendor roundups explain about those differences. Use that gap to your advantage. Ask each vendor to walk through your specialty from intake to payment posting, including where claims usually lose value and what controls they use to catch it.
A credible answer will include documentation triggers, payer-specific escalation rules, coding review checkpoints, and post-payment review logic.
2. Net collection performance, not just claim acceptance
Clean claims matter, but they are an input metric. CFOs need an output metric. Net Collection Rate comes closer to the financial question that matters: how much collectible revenue makes it into the bank.
This benchmarking analysis of medical billing company performance cites a high-performing Net Collection Rate range of 94% to 98%, while results below 90% often indicate material leakage. That gap usually does not come from one dramatic failure. It comes from many small ones, including weak follow-up, avoidable contractual write-offs, missed secondary billing, and underpayments that are posted as final.
Ask vendors what depresses NCR in your specialty. If they cannot connect NCR performance to payer mix, site of service, fee schedule variance, and underpayment recovery, they are measuring process quality more than financial performance.
3. A/R discipline and aging composition
A/R management should show control, not motion. A vendor can report thousands of touches and still allow balances to age into low-yield inventory.
Use aging composition to test operating discipline. Younger receivables convert faster, cost less to collect, and reveal whether the team escalates accounts while they are still recoverable. Older A/R often reflects unresolved payer behavior, weak documentation retrieval, or poor prioritization by balance and probability of recovery.
Ask for aging by payer, specialty, and place of service. Summary totals hide problem accounts.
4. Denial analytics tied to process correction
Denials are useful only if the vendor can trace them back to a controllable cause. A denial dashboard that stops at category counts does not help a practice improve reimbursement.
Strong vendors map denials to the actual failure point: eligibility, authorization, coding, documentation, modifier use, medical necessity edits, timely filing exposure, or payer policy drift. They also show how those findings changed front-end rules, coder review, and claim edits over time. The question is not whether they appeal denials. The question is whether denial data changes behavior upstream.
5. Underpayment recovery and payer-behavior intelligence
Weak billing models manifest when many vendors treat a paid claim as a completed claim, even when reimbursement lands below contract terms, below expected payer behavior, or below a defensible out-of-network position.
Underpayment control requires more than spot checks. It requires expected-allowed logic, payer rule tracking, variance thresholds, and a workflow for deciding which shortfalls deserve reconsideration, appeal, or formal dispute. This is especially important in specialties where the payer rarely denies outright and instead reduces reimbursement through repricing logic, code edits, or partial allowances that appear routine at posting.
Ask for examples. Which underpayments do they flag automatically? How do they distinguish contractual variance from payer error? What percentage of recovered cash comes from post-payment work rather than initial claim acceptance? Vendors that cannot answer those questions usually normalize avoidable loss.
6. IDR capability and dispute engineering
For specialties affected by the No Surprises Act, IDR capability belongs inside vendor evaluation, not in an afterthought. A billing company may be competent at charge entry, coding, and denials and still leave material revenue unprotected if it cannot identify eligible disputes, preserve timelines, assemble support, and connect payment variance to an IDR filing strategy.
The operational point is easy to miss. Winning disputes often depends on work done before the dispute exists. Documentation quality, coding precision, payer correspondence, qualifying payment amount analysis, and evidence retention all shape the quality of the file. If those functions sit in separate silos, the practice loses time and advantage before the case is even reviewed.
Test this directly. Ask the vendor to describe the evidence packet it builds for a disputed underpayment, who owns timeline control, and how payment posting triggers escalation.
7. Executive visibility and pricing discipline
Reporting should help a CFO identify margin risk by payer and service line. Generic dashboards that emphasize charges entered, claims submitted, or call volume rarely show where reimbursement is eroding.
Contract structure matters too. Percentage-of-collections pricing can hide weak post-payment recovery if the vendor gets paid on whatever the payer decides to remit. A better evaluation asks how compensation aligns with underpayment detection, aged A/R cleanup, dispute support, and visibility into recoverable revenue that would otherwise be written off.
Use this scorecard when comparing finalists:
| Framework point | What to ask for |
|---|---|
| Specialty depth | A workflow map for your specialty, including payer-specific risks |
| NCR performance | Trend reporting tied to collectible revenue, not just claim acceptance |
| A/R discipline | Aging by payer, place of service, and specialty code family |
| Denial analytics | Root-cause reporting linked to process changes |
| Underpayments | Method for identifying and recovering approved-but-underpaid claims |
| IDR readiness | Eligibility screening, evidence handling, and escalation ownership |
| Reporting and pricing | CFO-level visibility and contract terms tied to accountability |
The strongest firms operate like reimbursement control systems. They do not stop at submitting claims. They monitor what payers pay, identify where value leaks after adjudication, and build the documentation needed to recover it.
A Checklist for Specialty Practices and ASCs
A sales process should answer one question for a specialty CFO: where will this vendor protect collectible revenue after the claim is filed? That standard changes the evaluation. Many billing companies can produce clean claims and acceptable first-pass metrics. Fewer can show disciplined control over underpayments, payer-specific reimbursement variance, old A/R recovery, and dispute escalation for cases that fall into IDR or similar post-payment workflows.
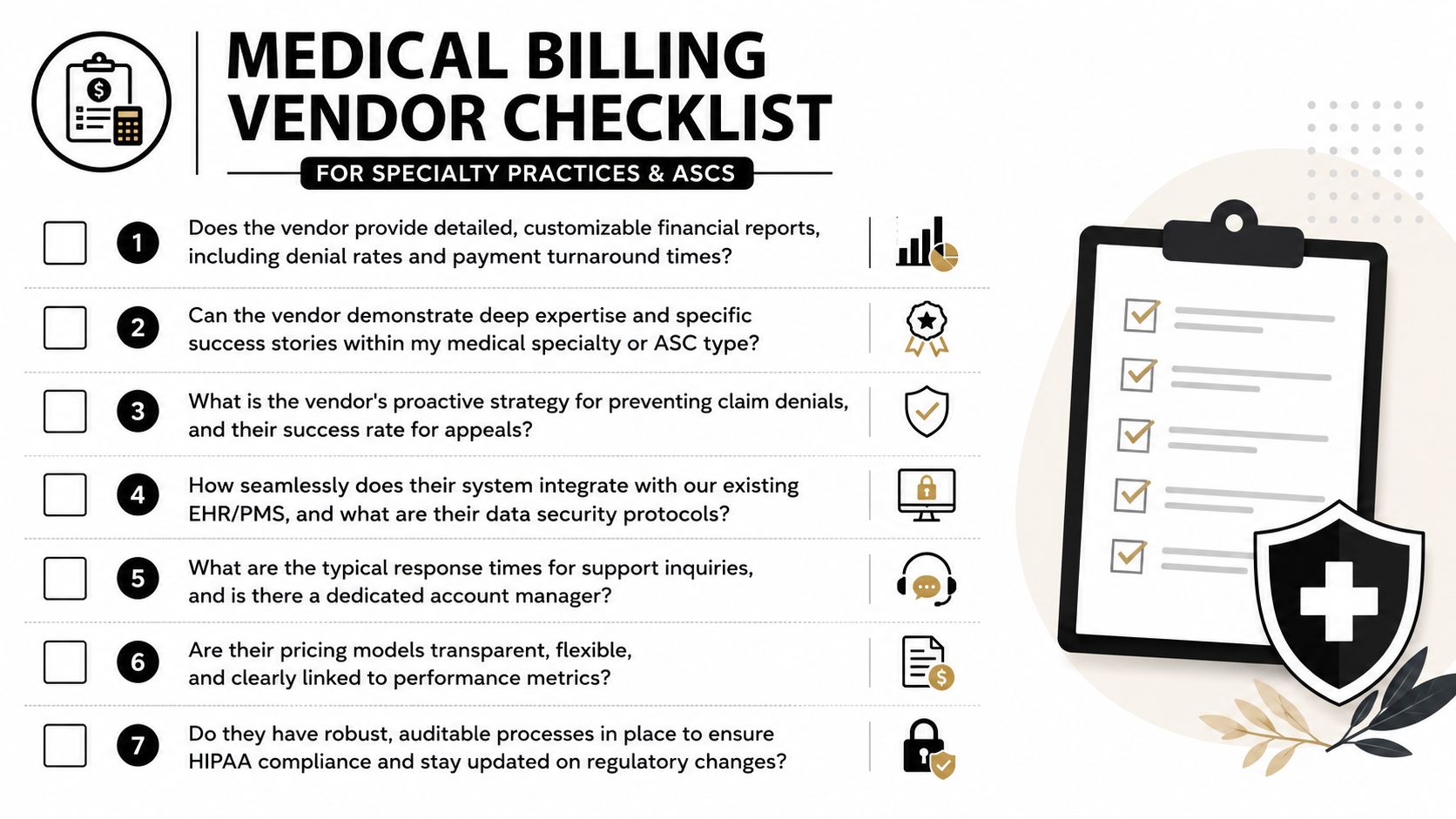
Questions that expose real capability
Broad prompts produce polished but low-value answers. Ask for evidence tied to operating discipline and recoverable dollars.
- Show me your A/R aging composition: Ask for aging by payer, location, and specialty, with a clear explanation of how the team works balances over 120 days. If they only show total A/R, they are hiding where collections slow down.
- Walk me through your workflow for my specialty: Ask how the process changes for anesthesia, orthopedics, air ambulance, GI, or dermatology. The right answer should include payer edits, coding risks, documentation triggers, and post-payment review rules specific to that service line.
- Describe your underpayment process: Ask how expected reimbursement is calculated, how payment variance is flagged, who reviews it, and what recovery path follows. A vendor that stops at payment posting will miss approved claims paid below contract, fee schedule, or statutory expectations.
- Explain your dispute path: For NSA-exposed specialties and ASCs, ask who screens cases for eligibility, who assembles supporting documentation, and who owns escalation if payer negotiations fail. If the answer collapses appeals and IDR into one vague process, capability is probably thin.
- Show me payer-level root-cause reporting: Ask for examples that separate authorization failures, coding edits, bundling behavior, medical necessity denials, and underpayment patterns. Those categories drive different fixes and different financial outcomes.
- Map your handoffs: Ask where eligibility, coding, charge capture, claim submission, posting, patient billing, appeals, and dispute support change hands. Leakage usually appears at the transition points, especially when one team closes a task before the next team accepts ownership.
- Tell me what you will not own: This question often produces the clearest answer. It shows whether the firm excludes legacy A/R, contract modeling, low-balance follow-up, complex appeals, or IDR preparation.
Red flags that deserve immediate attention
Some weaknesses appear before implementation. Others show up in the first month of reporting.
A vendor that answers every performance question with clean-claim rates is steering the discussion away from reimbursement quality.
Watch for these patterns:
- Generic specialty positioning: They claim broad experience but cannot describe specialty-specific reimbursement risks.
- Production-heavy dashboards: Their reports focus on claim volume, touches, and call counts instead of net collection performance, payment variance, and aged recoverables.
- Limited post-payment controls: They can explain denials but not approved claims paid short.
- Unclear dispute ownership: They mention appeals but cannot define decision rules, evidence standards, or escalation steps for formal dispute resolution.
- Inadequate old A/R strategy: They treat aging as a reporting category rather than a recovery workstream with payer-specific tactics.
- Pricing that rewards passivity: Percentage-of-collections models can work, but ask whether the fee structure creates any incentive to identify underpayments or pursue labor-intensive disputes.
One more caution matters for ASCs. A vendor may look strong in office-based professional billing and still struggle with facility claims, implant carve-outs, device-intensive cases, or payer policies that differ by place of service. Ask for examples from settings that match your revenue mix.
What to request before signing
Proposals do not show execution quality. Operating artifacts do.
- A sample executive dashboard with payer, specialty, place-of-service, and aging views.
- A sample denial analysis that traces root causes to process changes and financial impact.
- A sample payment variance report that shows how the team identifies underpaid claims after adjudication.
- A sample dispute workflow with decision points for appeal, negotiation, and IDR support where applicable.
- A transition plan with functional ownership, system dependencies, and reporting milestones.
- A recovery example from old A/R or underpayment inventory that shows how the vendor prioritizes effort against collectible value.
The goal is not to test presentation skills. It is to verify that the vendor has a repeatable reimbursement control process, especially after the payer issues payment. That is where a meaningful share of specialty revenue is still lost.
Quantifying the ROI With Real-World Scenarios
The return on the right billing partner usually appears in categories, not slogans. Specialty leaders should model value by asking where the current process loses collectible dollars: coding precision, denials, aging, underpayments, or unresolved disputes. The scenarios below stay qualitative because vendor-specific outcomes vary, but they reflect the kinds of recoverable value finance teams should look for.

Scenario one, anesthesia group with recurring downcoding
An anesthesia group may submit technically sound claims and still experience reimbursement pressure if payers repeatedly reinterpret time units, medical direction logic, or documentation sufficiency. A generic billing vendor often treats those payments as complete once they're posted. A stronger partner flags the pattern, compares expected versus actual payment behavior, and creates a structured response.
The ROI here comes from reclaiming amounts that would otherwise remain invisible. The practice doesn't need more patient volume. It needs a billing company that recognizes when “paid” doesn't mean “paid correctly.”
Scenario two, air ambulance operator facing NSA dispute exposure
Air ambulance reimbursement is shaped by federal rules, documentation standards, and high-stakes post-payment conflict. In that environment, traditional billing support covers only part of the problem. The bigger financial question is whether the claim was built to survive scrutiny and whether the team can escalate effectively when reimbursement comes in below defensible value.
The highest-value billing partner for dispute-heavy specialties is often the one that can prove what should happen after adjudication, not just before it.
The ROI in this scenario comes from connecting front-end claim engineering to back-end dispute readiness. Without that connection, the operator may collect something, but still leave substantial reimbursement value on the table.
Scenario three, orthopedic ASC with aging and payer variance issues
An orthopedic ASC may not be suffering from dramatic denial volume. Instead, the leakage may show up as aged balances, uneven payer follow-up, or partial payments that no one systematically reviews. A stronger billing company changes the economics by tightening coding turnaround, segmenting A/R aggressively, and assigning accountability for variances that weaker teams would classify as routine.
That creates several forms of return at once:
- Better cash timing: Younger receivables improve predictability.
- Cleaner payer accountability: Recurrent payment issues become visible instead of anecdotal.
- Stronger decision support: Leadership can see whether the issue is documentation, payer behavior, or internal process design.
The common pattern across these examples is simple. The ROI from medical billing companies isn't just collections uplift. It's the conversion of unmanaged reimbursement friction into a disciplined recovery process.
Choosing Your Revenue Protection Partner
The market itself is signaling that older billing models are under pressure. The number of medical billing businesses in the United States fell by 3.4% per year from 2019 to 2024, leaving 1,364 firms remaining, according to industry trend data summarized here. That decline suggests a shakeout. Generalist vendors and thin-service models are struggling to keep pace with payer complexity, specialty expectations, and the need for more advanced reimbursement oversight.
For specialty CFOs, that trend should sharpen the selection standard. The fundamental choice isn't between outsourcing and insourcing alone. It's between a vendor built for task execution and a partner built for revenue defense. Those are not the same thing. One helps claims move. The other helps reimbursement hold.
What the winning profile looks like
The strongest medical billing companies now share a few traits:
- They understand specialty economics: They don't force every service line into the same workflow.
- They measure financial reality: They report on collectible revenue, aging quality, and payment behavior.
- They don't stop at denials: They investigate underpayments and build escalation paths.
- They integrate compliance into operations: They don't treat NSA or dispute readiness as side issues.
- They give leadership visibility: Their reporting helps operators make decisions, not just review activity.
The decision that matters most
A low fee can be expensive if it buys shallow follow-up, generic coding oversight, and no path to recover approved-but-underpaid claims. A more capable partner may cost more on paper while protecting materially more revenue in practice. That's the comparison that matters.
If you're evaluating medical billing companies for a specialty practice, ASC, hospital service line, or multi-state platform, choose the firm that can explain your payer reality in operational detail. Ask how they protect reimbursement after adjudication. Ask how they handle underpayments. Ask when they escalate. Ask what evidence they preserve before a dispute starts.
The future of billing belongs to firms that combine claim production with payment enforcement. In a hostile payer environment, that isn't a premium feature. It's the baseline for financial resilience.
If your organization needs a billing partner that treats underpayments, payer behavior, and dispute readiness as part of one operating model, consider RevGuard. It combines specialty-focused RCM with IDR support under the No Surprises Act, which makes it relevant for practices and providers that can't afford to stop at clean claims alone.