
A payer just held a facility claim, your billing team says the coding looks fine, and cash you expected this month is now sitting in limbo. That's a familiar problem in hospitals, ASCs, rehab centers, and other institutional settings. The issue often isn't one dramatic error. It's one field, one status code, one revenue line, or one mismatch that changes how the payer reads the entire encounter.
That's why the answer to what is a UB-04 form matters far beyond billing operations. For an institutional provider, the UB-04 isn't routine paperwork. It's the record that tells the payer what happened, why it was billable, how the stay or visit should be classified, and how payment should be calculated. If that story is incomplete or inconsistent, reimbursement gets delayed, reduced, or denied.
The other reason this matters now is disputes. When a payer underpays or challenges a facility claim, the UB-04 becomes part of the evidence trail. If the form is clean, consistent, and supported by the chart, you have a much stronger position. If it's sloppy, every downstream appeal gets harder.
What Is the UB-04 and Why Does It Matter
The UB-04, also called CMS-1450, is the standard claim form used by institutional providers to bill facility services. It's built for places like hospitals, nursing homes, and ASCs, not for an individual physician's professional fee.
That distinction matters because institutional billing is operationally dense. A facility claim may need to reflect admission details, discharge status, multiple departments, room charges, ancillary services, and payer-specific billing logic. The UB-04 gives payers a uniform way to process all of that.
According to MedStates' overview of the UB-04 form, the form is designed specifically for facility-based providers such as hospitals, nursing homes, and ASCs. That same source notes that roughly 70 to 80% of institutional claims in the United States not submitted electronically are still processed from the paper UB-04, and that Medicare and Medicaid guidance explicitly mandates its use. The practical takeaway is simple. This form still sits at the center of institutional reimbursement.
Why revenue leaders care about a “simple form”
Most new practice managers first see the UB-04 as a billing artifact. Experienced revenue cycle leaders see it differently. They see it as the translation layer between clinical activity and payment.
If the translation is wrong, several things happen fast:
- Claims suspend or deny: Payers can't reconcile the billed services with the claim structure.
- Payment logic changes: The wrong bill type or discharge status can send the claim down the wrong adjudication path.
- Appeals get weaker: You spend time arguing over issues that should've been correct at first submission.
- Compliance risk rises: Inconsistent facility billing invites deeper payer review.
Practical rule: Treat the UB-04 as a financial document with compliance consequences, not as a form your team completes at the end.
For facilities operating under thin margins, that mindset changes behavior. Teams pay closer attention to registration, utilization review, coding, charge capture, and claim edits because they know all of it surfaces on the UB-04.
Anatomy of the UB-04 Claim Form
The UB-04 is the standard institutional claim form approved by the National Uniform Billing Committee. It replaced the older UB-92 after NUBC approval in 2005, and it contains 81 numbered data fields called Form Locators, according to AHIMA's key points on the UB-04 update. That same AHIMA document explains that the data set aligns with the HIPAA ASC X12N 837 Institutional standard, which is why the same core information can move through paper and electronic institutional billing workflows.
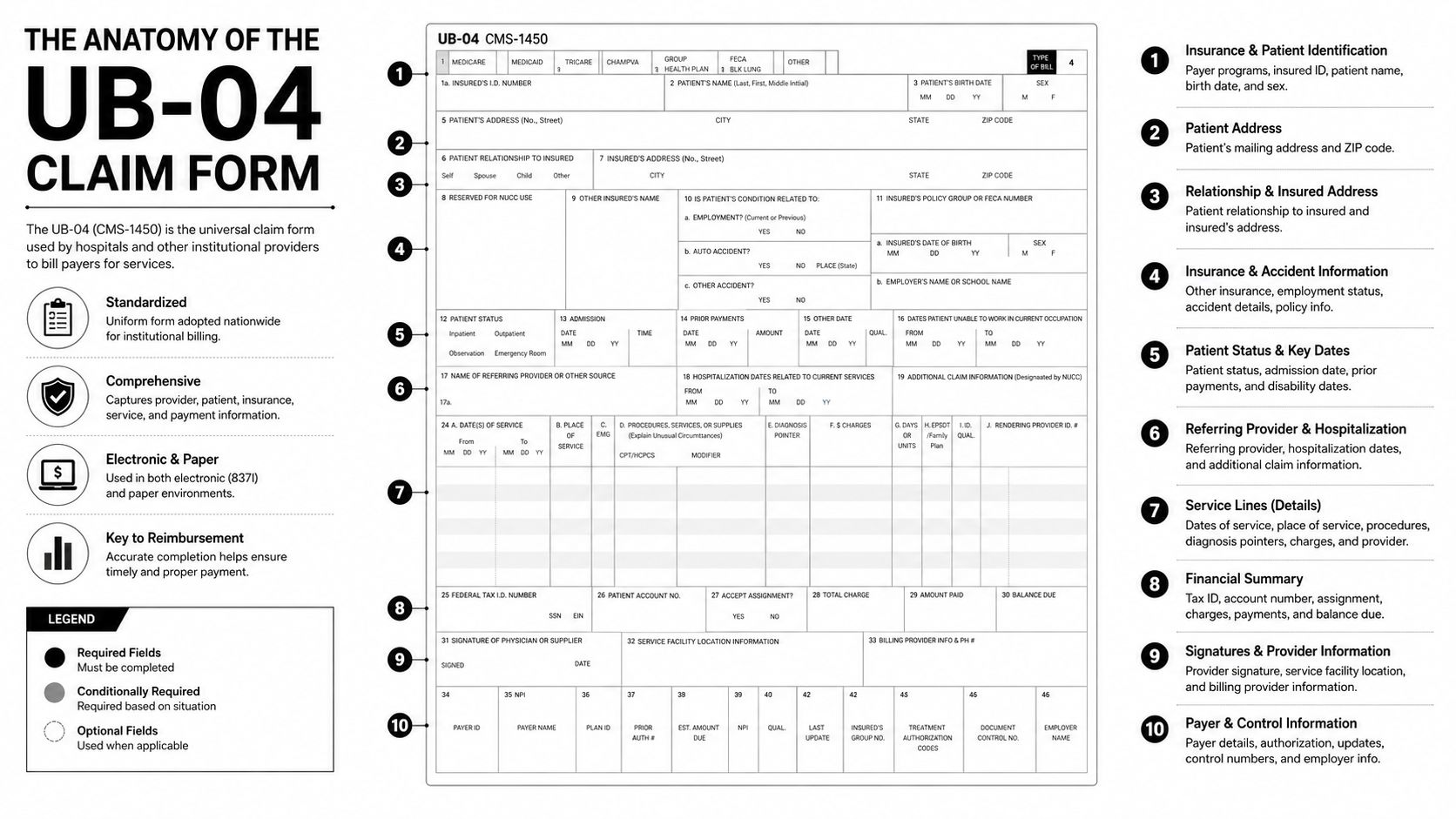
What the form is built to capture
At a practical level, the form captures the major ingredients of a facility claim:
- Facility identity: Who is billing and under which institutional structure
- Patient and encounter details: Dates, demographics, admission information
- Service categorization: Department-level lines through revenue coding
- Clinical justification: Diagnosis data that supports medical necessity
- Billing classification: The logic that tells the payer how to interpret the encounter
Think of the UB-04 as the passport for the facility claim. It tells the payer where the claim came from, what kind of institutional service it represents, and how it should travel through adjudication.
UB-04 versus CMS-1500
This is the confusion point that causes real operational mistakes.
The UB-04 tells the story of the facility. The CMS-1500 tells the story of the professional. If an anesthesiologist, surgeon, or consulting physician is billing professional services, that typically belongs on the physician-oriented claim form. If the hospital or ASC is billing the facility portion of the encounter, that belongs on the UB-04.
A simple comparison helps:
| Form | Primary use | Typical biller |
|---|---|---|
| UB-04 / CMS-1450 | Institutional or facility charges | Hospitals, ASCs, SNFs, rehab facilities |
| CMS-1500 | Professional services | Physicians and other individual practitioners |
That separation affects workflow, coding review, and denial management. Teams that blur it usually create avoidable rework.
Where revenue codes fit
One of the most important structural parts of the form is the revenue code area. Revenue codes identify the department or service category tied to the charge line and shape how a payer interprets the institutional claim. If your team needs a deeper primer, this guide on what revenue codes do in facility billing is a useful companion to understanding the UB-04 layout.
A clean UB-04 doesn't happen in the billing office alone. Registration, case management, coding, and chargemaster governance all leave fingerprints on the final claim.
Decoding Critical UB-04 Form Locators
You don't need to memorize all 81 Form Locators to manage institutional reimbursement well. You do need to know which ones carry the most operational risk. In practice, a small set of fields drives a large share of claim edits, payment variances, and dispute headaches.
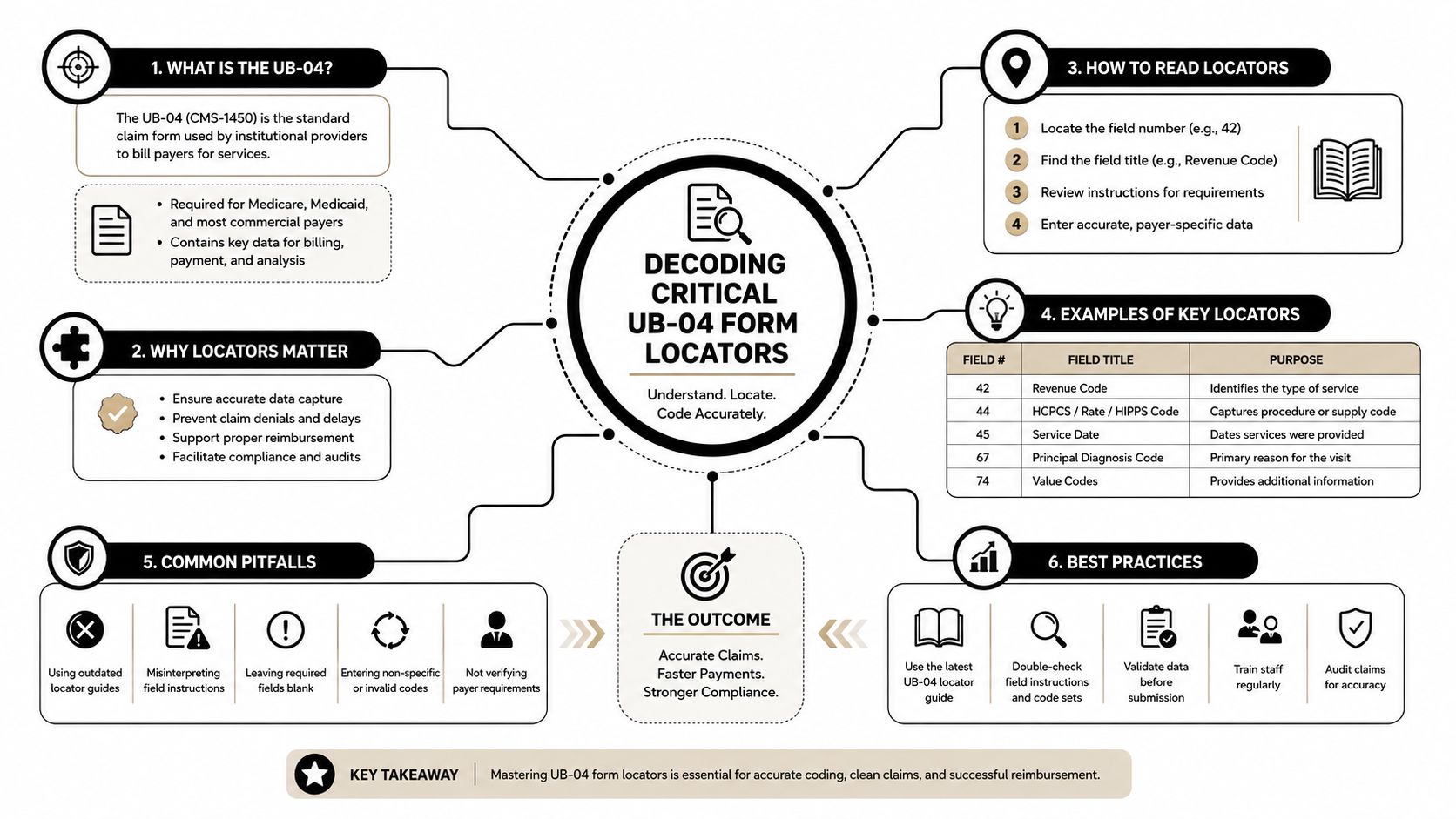
FL 4 and the claim's basic identity
Form Locator 4, the Type of Bill, is one of the first fields I review when a claim denial doesn't make sense. It tells the payer what kind of facility bill it is and influences the adjudication path from the start.
The verified background on the UB-04 notes that the form supports consistent capture of Type of Bill values such as 111 and 121 within its standardized data set. That matters because payers don't read these codes as labels. They read them as instructions. A wrong bill type can turn a valid claim into a mismatch before the system even evaluates the clinical details.
If your billing team keeps correcting downstream denials, start upstream with FL 4. The claim may be “accurate” in a general sense and still be structurally wrong.
FL 14 and FL 17
FL 14, the priority or type of admission, helps define how the encounter began. FL 17, patient discharge status, helps define how it ended. Those fields are easy to underestimate because they don't look like charge lines. But they affect how the payer interprets the stay, especially in facility settings where admission source and patient status matter.
AHIMA's UB-04 update notes that the form supports discharge status reporting with over 50 standardized codes in the institutional data set. That tells you two things. First, status reporting is not casual data entry. Second, there's enough specificity built into the form that vague or assumed coding won't hold up.
When a payer questions the shape of an encounter, not just the charge, they often start with admission and discharge fields.
FL 42 through FL 49
Many facility claims become persuasive or fall apart depending on these locators. These locators carry the line-level financial narrative: revenue codes, service dates, units, rates, and charges.
The UB-04's design supports multiple revenue codes tied to service lines such as operating room, imaging, and laboratory functions, as described in the verified background on institutional billing. That's why line integrity matters so much. A facility claim isn't just “a surgery” or “an outpatient visit.” It's a set of categorized services that must make sense together.
Three practical failure points show up repeatedly:
- Revenue code and service mismatch: The line doesn't reflect the department or category where the service belongs.
- Charge capture inconsistency: The chart shows activity that the claim doesn't express clearly.
- Unsupported units or dates: The line item doesn't align with the service documentation.
FL 67 and the diagnosis anchor
FL 67, the principal diagnosis code, is the clinical anchor of the claim. It doesn't just describe the patient's condition. It helps justify why the facility services on the claim were necessary and how the entire billed encounter should be understood.
When FL 67 and the service lines don't support each other, the payer has an opening. They may challenge medical necessity, coding accuracy, or the billed structure itself. Even when the claim isn't denied outright, this kind of inconsistency can trigger review and delay.
A practical reading sequence
When you audit a UB-04, don't read it from top to bottom like a static form. Read it like a payer system:
- Start with bill identity in FL 4.
- Confirm the encounter shape through admission and discharge details.
- Review revenue lines for internal consistency.
- Check diagnosis support for the billed services.
- Compare the claim story to the chart story.
That sequence catches more meaningful issues than checking boxes one by one.
The UB-04 Lifecycle from Submission to Payment
A UB-04 claim doesn't become a revenue event when the patient is discharged. It becomes a revenue event when the facility translates the encounter correctly, validates it, submits it, and gets it through payer adjudication without avoidable friction.
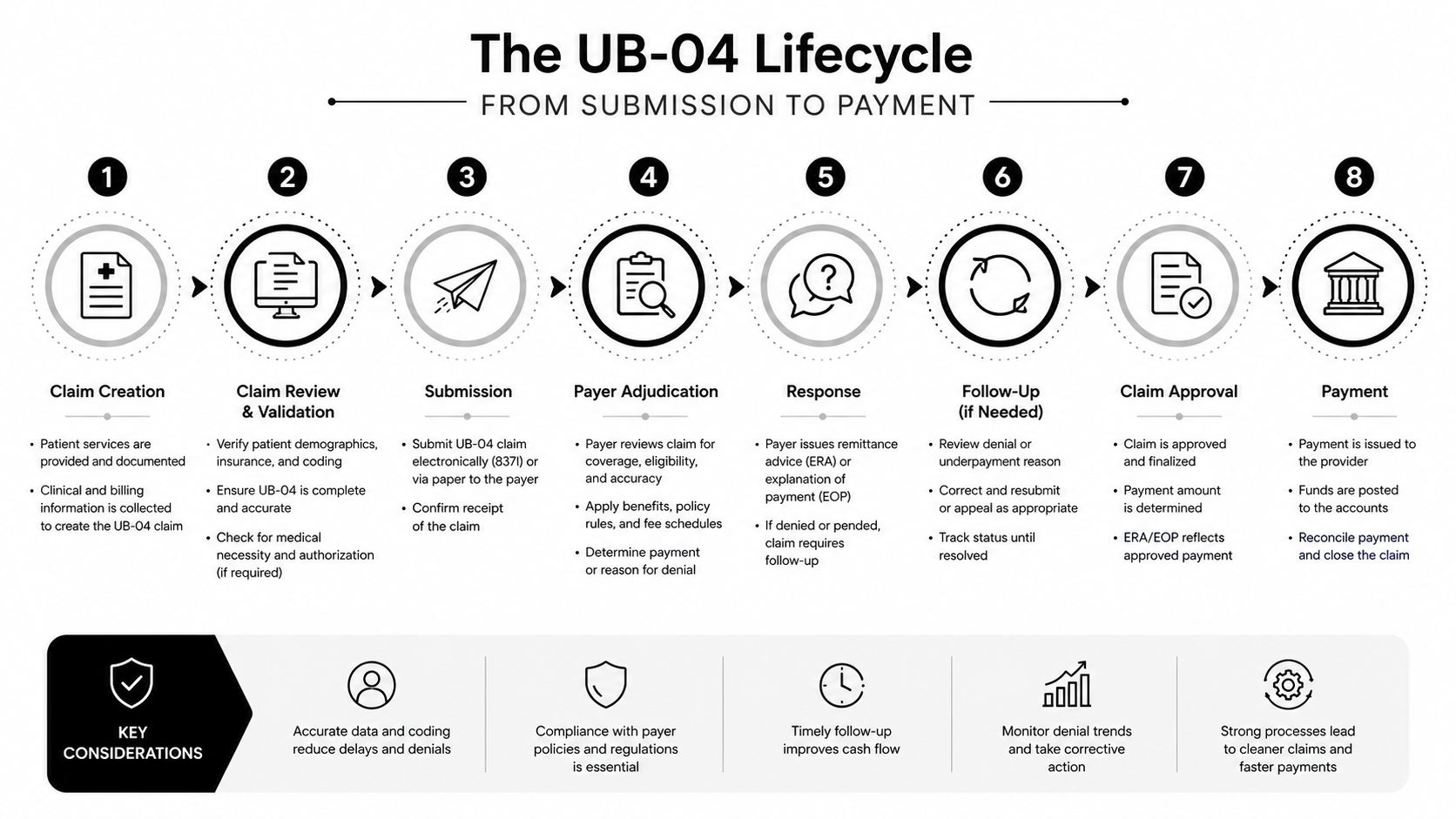
How the claim actually moves
The lifecycle usually starts well before claim creation. Registration captures patient and insurance details. Clinical teams document the encounter. Coding translates the record. Charge capture pulls in the billable facility activity. Then the billing system assembles the institutional claim.
At that point, the claim should go through edits and scrubbing. During these processes, your team catches missing data, invalid combinations, payer-specific requirements, and obvious logic conflicts. If you skip this discipline, you push basic errors into the payer's system and turn clean-up into expensive rework.
The institutional claim may be submitted on paper UB-04 in some cases, but the same data can also flow electronically through the 837I format. The key point isn't the medium. It's whether the data package is complete and coherent.
What payers do with it
Once submitted, the payer doesn't “review the claim” the way a human revenue cycle manager would. Their systems sort, validate, and adjudicate based on the claim fields and plan rules. The software checks whether the billed structure fits what that payer expects for the member, benefit design, provider type, and service category.
If the claim passes those checks, adjudication moves toward payment. If it doesn't, the payer may reject, deny, pend, or underpay. Those are different outcomes operationally, but they all create the same business problem. Your facility doesn't have the cash yet.
For newer managers, understanding the remittance side is just as important as understanding submission. This primer on how an EOB fits into medical billing workflows helps connect the UB-04 you send with the explanation you receive back.
Where good teams intervene
Strong teams don't wait for the remittance to discover what went wrong. They build control points before submission and right after payer response.
A practical operating model looks like this:
- Before submission: Validate registration, bill type, diagnosis support, and line-level revenue coding.
- At submission: Track acceptance at the clearinghouse and payer intake level.
- After adjudication: Separate true denials from underpayments, processing errors, and documentation issues.
- During follow-up: Work from root cause, not just claim status notes.
Clean claim performance improves when billing staff stop treating every payer response as the same problem.
That shift matters because a rejected claim needs correction, a denied claim may need appeal, and an underpaid claim may require a payment dispute strategy.
Common UB-04 Errors That Trigger Denials
Most UB-04 denials aren't mysterious. They're predictable. The frustrating part is that facilities often see the same patterns over and over because the root cause lives upstream in registration, coding, utilization review, or charge capture.
Problem patterns that cost facilities money
Here are the UB-04 mistakes I'd put on any manager's watch list.
Wrong Type of Bill
The payer processes the claim under the wrong institutional category or frequency logic. That can derail the claim before medical necessity is even considered. The fix is governance, not heroics. Maintain a current bill type matrix by service setting and teach staff when corrected claims require a different billing path.
Discharge status that doesn't match the record
The claim tells the payer the patient left under one status, while the chart and downstream care record suggest another. That inconsistency invites denial, delay, or recoupment risk. The solution is tighter coordination between case management, HIM, and billing before final claim release.
Revenue code errors
A line may be missing a needed revenue code, using the wrong departmental category, or presenting a set of lines that doesn't make sense together. Since revenue lines help define the facility story, bad line construction weakens the whole claim. Review chargemaster mapping and pre-bill edits instead of correcting one-off denials forever.
Mismatches that payers catch quickly
Some issues are simple and still expensive.
| Problem | Why it causes trouble | Better practice |
|---|---|---|
| Diagnosis and procedure mismatch | The clinical rationale doesn't support the billed service pattern | Reconcile coding and final claim review before release |
| Patient demographic or coverage error | The payer can't match the member or plan correctly | Tighten front-end registration and eligibility checks |
| Dates that conflict | Service timing, admission, or statement period doesn't line up | Validate encounter timeline before submission |
What works and what doesn't
What works is a pre-bill review model that focuses on high-risk fields, not a generic checklist that treats every claim the same. For example, inpatient, outpatient surgery, observation, and rehab claims do not fail in identical ways. Your edits should reflect that.
What doesn't work is relying on billers to fix everything after discharge with limited context. Once the claim is built from flawed source data, the billing office is often choosing between imperfect options.
The fastest denial to resolve is the one your team prevented before the claim ever left the building.
Another mistake is overcorrecting toward payer preference without checking compliance. Facilities sometimes alter claim construction to “get it paid” even when the chart or billing rules don't support that change. That may solve one account and create a larger exposure later.
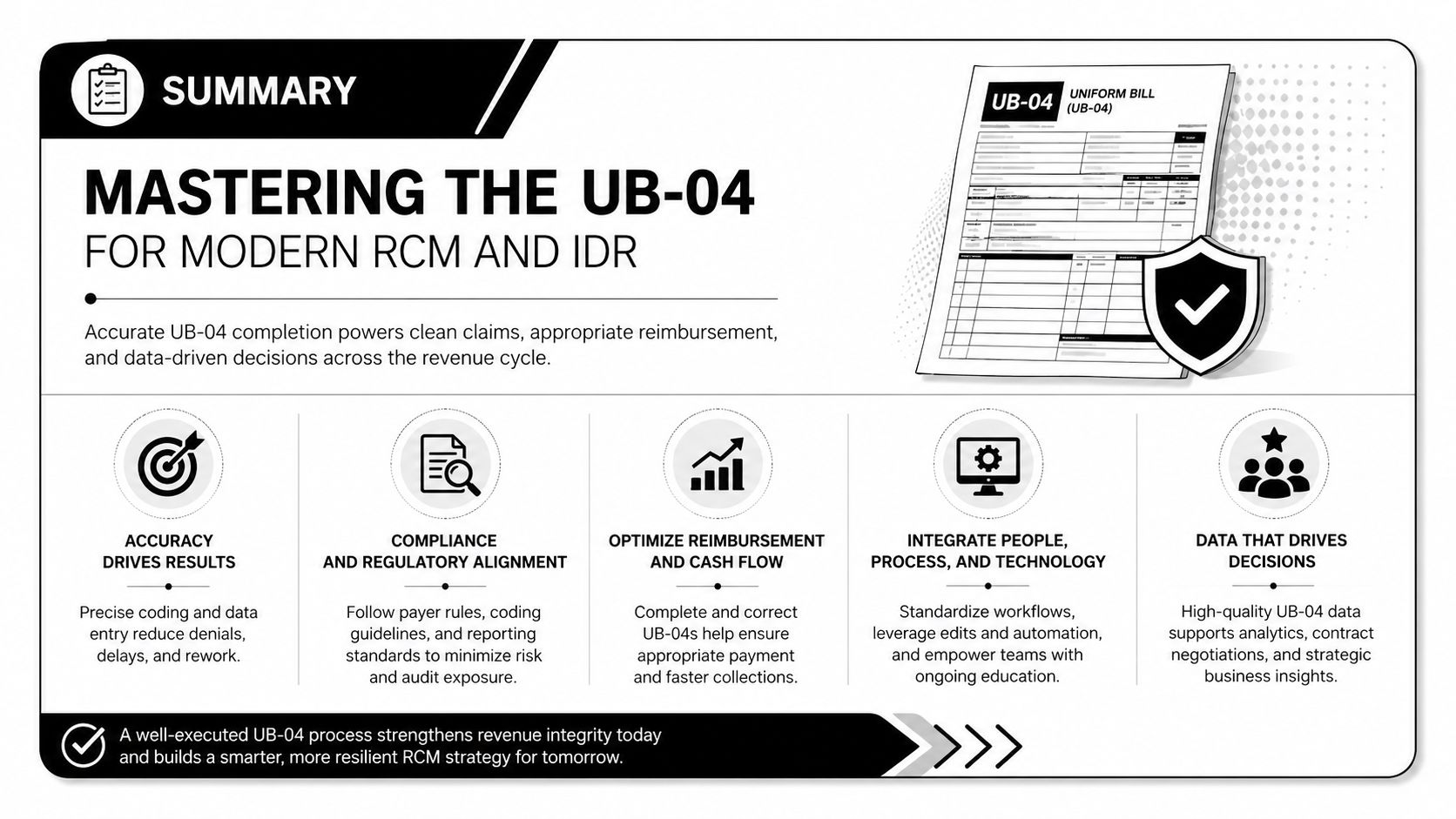
Mastering the UB-04 for Modern RCM and IDR
A well-built UB-04 does more than get a claim out the door. It protects revenue on the front end and strengthens your position when payment disputes begin. That's the part too many organizations miss.
Why the form matters in disputes
Under the No Surprises Act environment, facilities and provider groups can't afford to treat claim accuracy and payment disputes as separate departments with separate goals. The UB-04 often becomes part of the factual record that supports what was billed, how the encounter was classified, and whether the payer's reimbursement position makes sense.
If the claim form is internally consistent, supported by documentation, and coded in a way that reflects the actual institutional service, your appeal or dispute starts on solid ground. If the form contains preventable defects, the payer has more room to challenge the amount, the structure, or the legitimacy of the billed services.
That's especially important when teams pursue formal underpayment recovery. In those situations, every inconsistency becomes a credibility problem.
The modern operating standard
Revenue cycle teams need to think in two layers.
First, build clean, payable facility claims. That means disciplined registration, accurate coding, valid revenue line construction, and thoughtful claim edits.
Second, build dispute-ready claims. That means the claim should hold up when someone outside your organization examines it closely. Could a payer auditor follow the encounter? Could counsel understand the billing logic? Could an independent reviewer see why the facility billed what it billed?
That standard changes how you manage denials. Instead of asking only, “Can we get this paid?” ask, “Would this claim survive escalation?”
What strong organizations do differently
They don't isolate billing from denial strategy. They connect the two.
- They preserve claim integrity: Corrections are based on documentation and billing rules, not guesswork.
- They document the rationale: When unusual billing choices are necessary, staff record why.
- They separate coding issues from payer behavior: Not every short pay is a claim defect.
- They watch denial patterns by payer and service line: Repetition usually signals a system issue, not a one-off account.
If your team is rebuilding its process, a focused look at healthcare denial management workflows can help frame how UB-04 quality and dispute performance connect.
A clean UB-04 is not just a billing output. It is evidence.
That's the bottom-line issue. Facilities that master the UB-04 don't just reduce friction. They defend reimbursement more effectively when friction becomes conflict.
UB-04 Form Frequently Asked Questions
What changed when the UB-04 replaced the UB-92
The UB-04 became the successor to the older UB-92 after NUBC approval in 2005. It standardized institutional billing in the newer format and aligned the data set with modern electronic institutional claim workflows.
Can a UB-04 be used for professional fees
Generally, no. The UB-04 is for institutional or facility billing. Professional services billed by individual practitioners are typically reported on the physician-oriented CMS-1500 claim form.
Is the UB-04 only for hospitals
No. It's used by a range of facility-based providers, including hospitals, nursing homes, rehabilitation centers, home health agencies, and certain outpatient facilities.
Does paper UB-04 still matter if my team submits electronically
Yes. Even when your team submits through the electronic institutional transaction, the same core institutional claim content still matters. Operationally, the paper form remains useful as a reference model for how facility data is structured, reviewed, and audited.
If your organization needs help turning facility claims into cleaner payments and stronger underpayment disputes, RevGuard works across RCM and No Surprises Act IDR to help hospitals, ASCs, and specialty providers protect reimbursement with claims that are built to pay and built to hold up under scrutiny.