
You're probably staring at a queue of remits, patient statements waiting to go out, and aging balances that don't make sense. The payer says the claim processed. Your billing system says the encounter is still short. The front desk is fielding patient calls because the bill doesn't match what the plan told them. That's where staff often treat the EOB like paperwork.
That's a mistake.
In provider operations, the EOB in medical billing is not just a patient-facing explanation. It's one of your earliest usable signals that a payer has priced a claim correctly, priced it incorrectly, split it in an unexpected way, denied part of it, or shifted too much liability to the patient. Teams that only post from it stay reactive. Teams that analyze it build underpayment inventories, cleaner appeals, and stronger dispute files.
The EOBs Foundational Role in the Revenue Cycle
A payer sends payment on a claim your team expected to close cleanly. The money posts short. The patient balance looks inflated. If staff treats the EOB as a courtesy document instead of an adjudication record, that variance reaches A/R before anyone questions it.
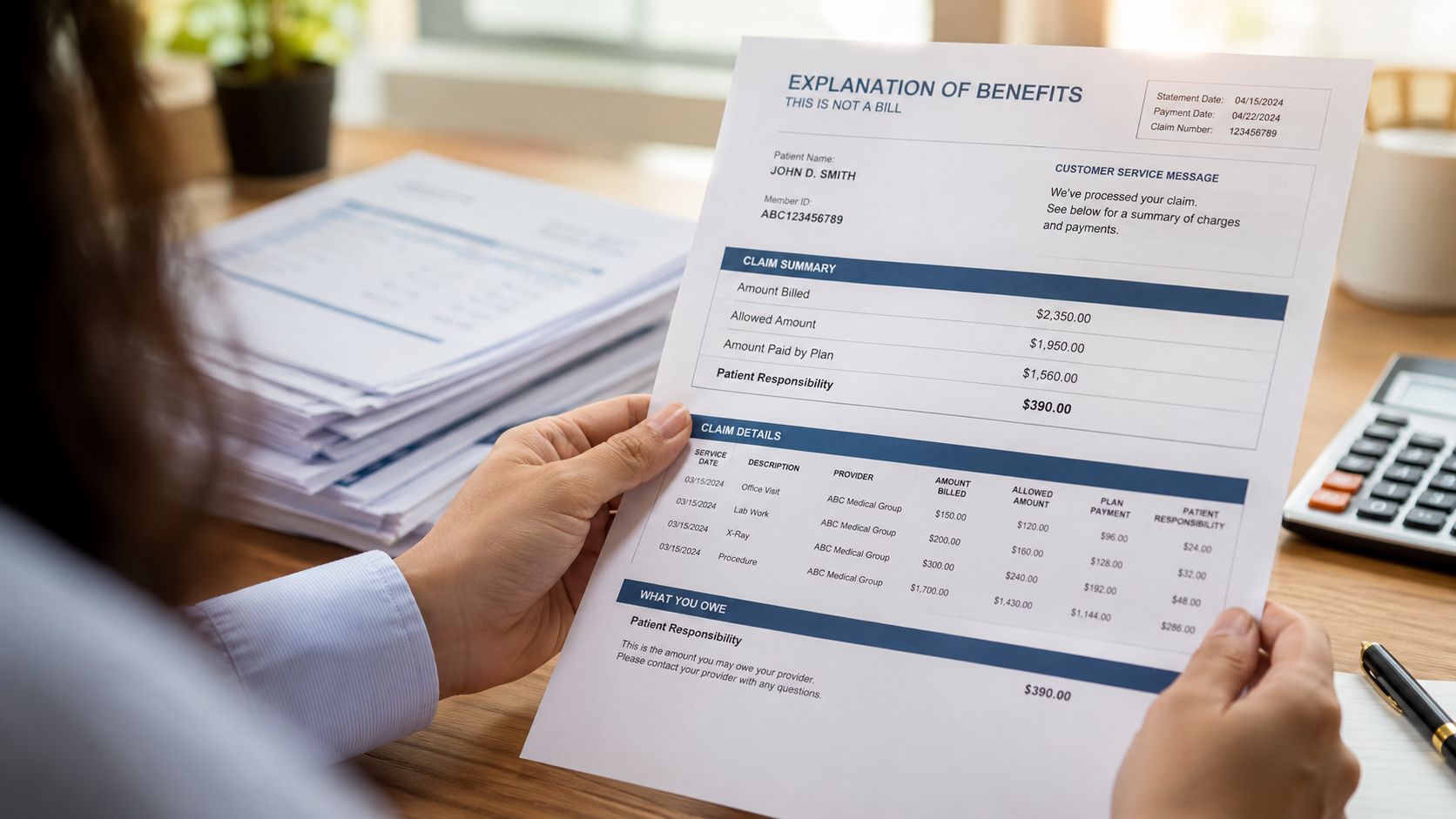
An Explanation of Benefits gives patients a summary of how the health plan processed the claim and what cost share may remain, as explained in CMS guidance on Explanation of Benefits. For providers, the same document serves a different purpose. It is the payer's written position on pricing, edits, denials, and liability allocation.
Why the EOB matters before patient billing
Before a statement goes out or a balance moves deeper into follow-up, the EOB should answer four operational questions:
- Did the payer adjudicate every billed line
- Did reimbursement match the contracted or expected allowed amount
- Did the payer apply reductions, bundling, or denial logic that needs review
- Did the payer assign patient responsibility correctly
That review protects two revenue points at once. It keeps the practice from writing off collectible dollars as contractual, and it keeps the practice from billing patients for balances the payer should have covered.
I tell new billing managers to treat the EOB as the first audit trail after adjudication. Once a bad allowance, unsupported adjustment, or misassigned coinsurance gets posted without review, fixing it takes more touches, more staff time, and usually more patient friction.
Practical rule: The patient statement should never be your first notice that the claim was processed incorrectly.
What strong revenue teams use it for
Experienced teams use the EOB as a control document, not a filing document. In day-to-day operations, it supports:
- Payment verification against fee schedules, case rates, expected out-of-network reimbursement, or other payer terms
- Variance detection when a payer prices one line, modifier, or unit differently from expectation
- Denial isolation so staff can separate partial denials from full-claim issues and route work correctly
- Patient balance validation before deductible, copay, or coinsurance is transferred to the ledger
- Appeal and dispute support because the EOB records the payer's adjudication outcome and stated rationale
That last point matters more than many teams realize. If underpayments repeat across the same codes, plans, or facilities, the EOBs stop being one-off payment notices. They become evidence. Patterns in EOB language, adjustment behavior, and reimbursement gaps help build appeal inventories, payer trend reports, and stronger IDR files when informal follow-up fails.
The operational shift that protects revenue
Billing offices lose margin when posters focus only on cash receipt. The better standard is to review EOBs as payer intelligence.
That means asking harder questions at the point of posting. Was the claim priced according to contract terms. Did the payer reclassify a service without support. Did the adjudication create patient liability that conflicts with plan rules or authorization facts. Is this an isolated variance, or the start of a repeatable underpayment pattern across the payer?
That is the EOB's foundational role in the revenue cycle. It documents how the payer decided the claim, and it gives your team the first usable record for catching underpayments before they settle into A/R as if they were correct.
How to Read and Interpret Key EOB Data
A strong biller can scan an EOB and understand the payer's logic within minutes. That skill comes from knowing which fields drive revenue and which fields merely describe the claim.
The EOB is generated after claims processing and reflects payer edits such as benefit verification, coverage determination, negotiated allowed amounts, and calculation of deductible, copay, and coinsurance, which is why it functions as a control document for underpayment and contractual variance, as described in this overview of EOB processing logic.
The fields that actually move money
Think of the EOB as the payer's financial receipt, but one written from the payer's perspective.
Here's the core anatomy:
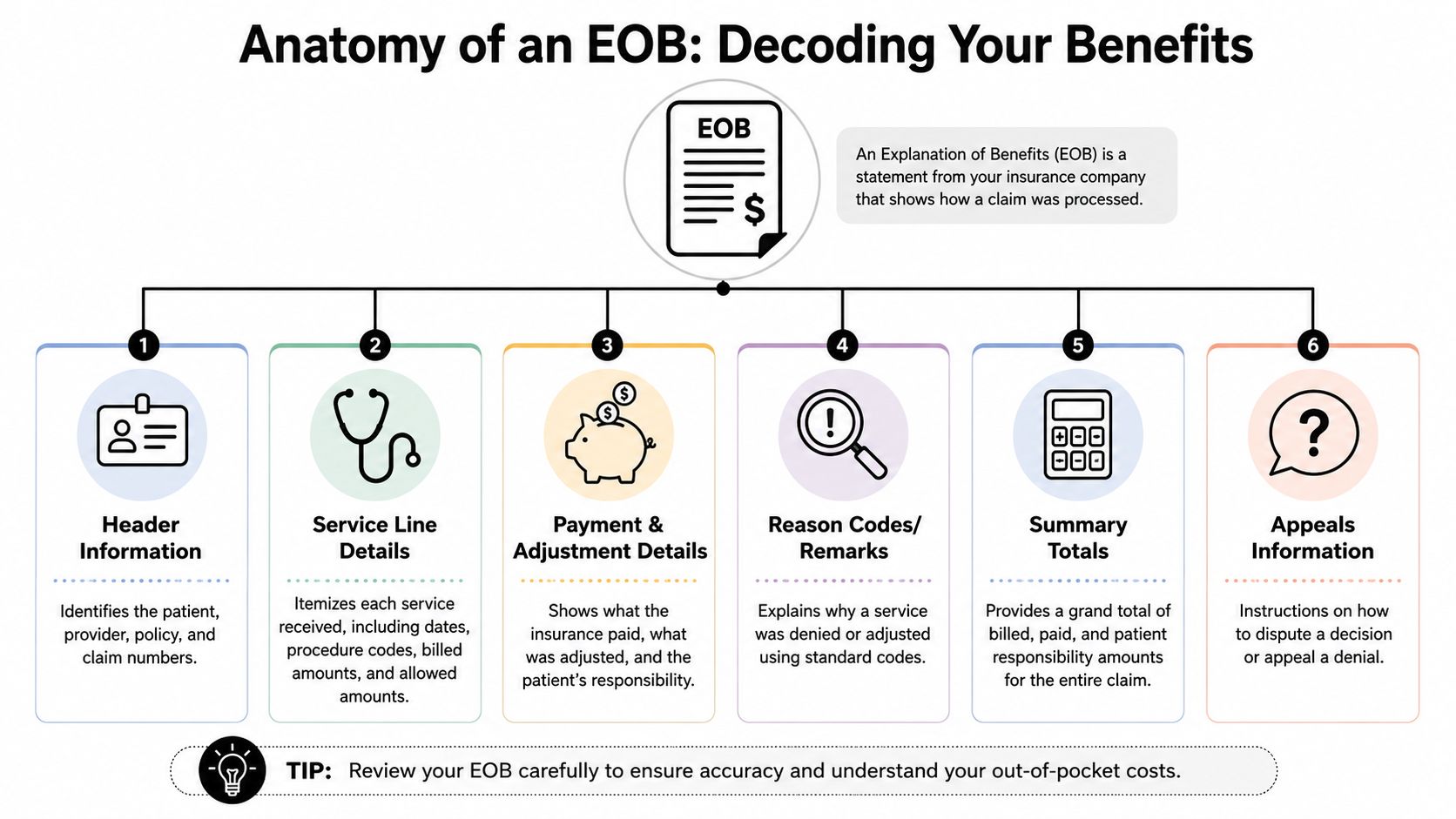
| EOB field | What it tells your team | Why it matters |
|---|---|---|
| Header information | Patient, provider, claim, and policy identifiers | Confirms you're matching the right remit to the right encounter |
| Billed charges | What your practice submitted | Establishes the starting point for reimbursement review |
| Allowed amount | What the payer recognizes under its pricing logic | This is where underpayment review usually starts |
| Adjustments | Amounts removed from the billed charge | Separates contractually expected reductions from questionable ones |
| Paid amount | What the payer actually sent | Needs to reconcile to posting and deposit workflow |
| Patient responsibility | Deductible, copay, coinsurance, or non-covered amounts | Drives patient statements and collection accuracy |
| Reason codes and remarks | Why the payer reduced, denied, or reclassified payment | Gives your team the roadmap for next action |
How to interpret it line by line
Don't read only the claim total. Read each service line.
A claim may look acceptable in summary and still hide a problem inside one procedure line, one modifier, one date of service, or one provider component. This is especially common when a payer pays part of the encounter and applies adjustments to the remainder under bundling logic or coverage edits.
Use this sequence:
- Start with the service date and procedure line. Make sure each billed line appears on the EOB.
- Check the allowed amount next. If your team doesn't know how to evaluate it, build that capability first. A practical primer on insurance allowed amount review helps frame what to compare.
- Review the adjustment reason before accepting the write-off. A write-off without a valid reason is how leakage gets normalized.
- Finish with patient responsibility. If the payer assigned the wrong patient balance, your collections team inherits a dispute you didn't create.
If your staff only posts totals, they're not reconciling. They're copying payer output into the ledger.
Red flags that deserve immediate review
Some EOBs should go straight into exception workflow:
- Missing service lines
- Unexpected non-covered designations
- Allowed amounts that don't match historical payer behavior
- Patient responsibility that feels disproportionate to the adjudication
- Adjustment codes that repeat across the same payer
Those aren't always payer errors. Sometimes they trace back to registration, coding, authorization, or claim construction. But the EOB is usually where you first see the damage clearly enough to act.
EOB vs ERA and Remittance Advice
Billing teams use these terms interchangeably, and that creates avoidable confusion in workflow design. They're related, but they aren't the same thing.
The simplest distinction
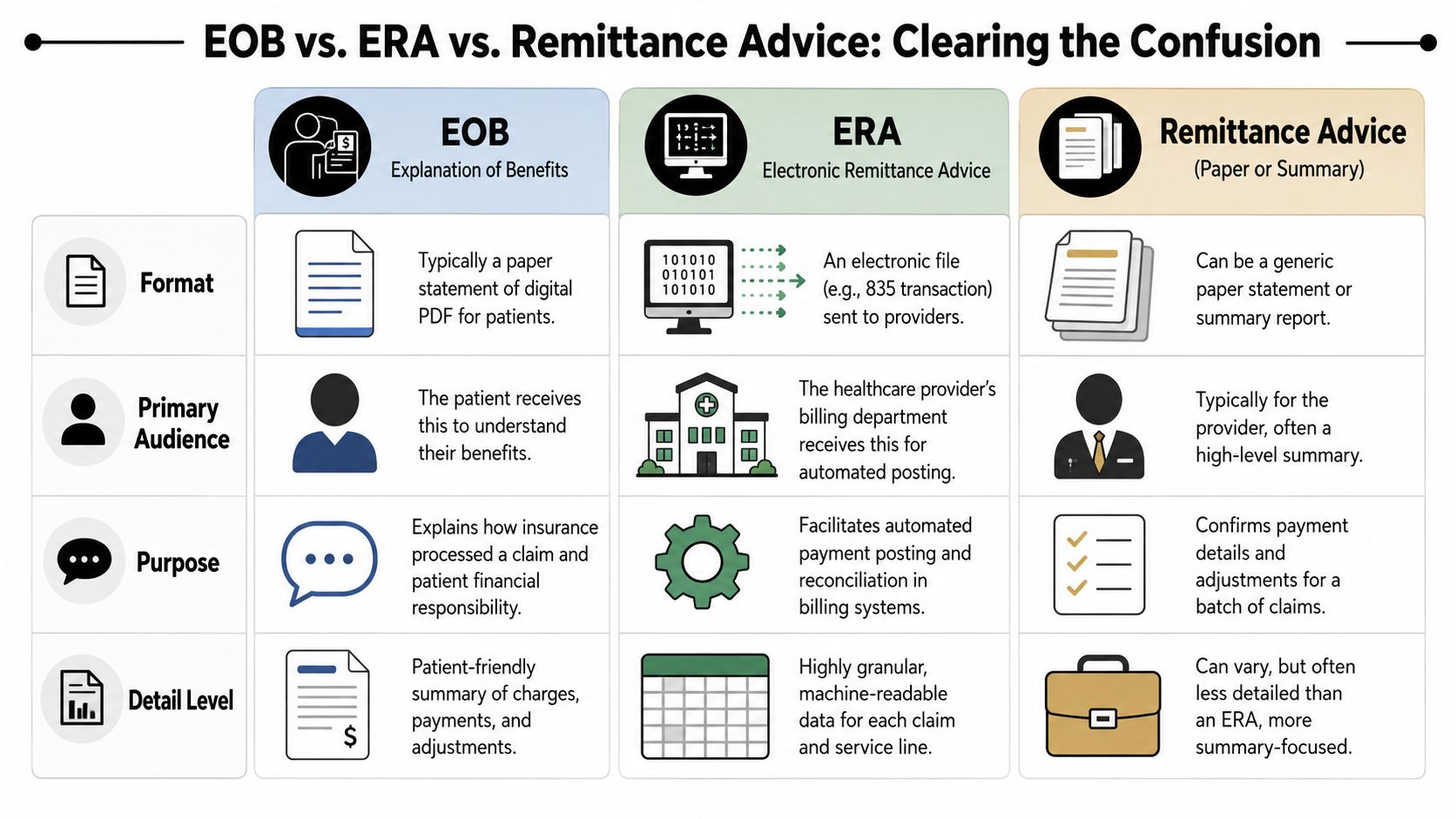
The EOB is typically the explanation sent to the patient. It explains how the claim processed and what financial responsibility remains.
The ERA is the electronic version used by providers for posting and reconciliation inside billing workflows. It carries structured adjudication data your system can ingest.
A remittance advice is the broader payment explanation from the payer to the provider. Depending on the payer and workflow, it may appear as a paper summary, a portal view, or an electronic transaction.
Side by side comparison
| Document | Primary audience | Typical format | Main operational use |
|---|---|---|---|
| EOB | Patient, but valuable to providers | Paper statement or digital PDF | Understand adjudication and patient liability |
| ERA | Provider billing team | Electronic remittance file | Automated posting and line-level reconciliation |
| Remittance advice | Provider | Paper or electronic summary | Payment confirmation and adjustment review |
Where teams get into trouble
Problems start when a practice trusts one document in isolation.
If staff rely only on the ERA, they may post efficiently but miss patient-facing inconsistencies that later trigger billing complaints. If they rely only on the EOB, they may understand the adjudication but still fail to reconcile payment movement cleanly inside the practice management system. If they look only at a high-level remittance summary, they can miss service-line variances.
A mature revenue cycle operation connects all three:
- The ERA drives system posting
- The remittance advice supports payment-level review
- The EOB validates how the payer communicated adjudication and member liability
The operational rule
Use the ERA for speed. Use the EOB for explanation. Use remittance advice to confirm what was paid and how it was grouped.
That combination keeps your team from making a common mistake. Accepting the payer's reduction as final just because the file posted cleanly.
A Practical Workflow for EOB Reconciliation
Most revenue leakage doesn't come from dramatic denials. It comes from unresolved mismatches that no one owns. One encounter generates multiple claims. One payment covers multiple dates. One facility and one professional component process separately. The EOB looks complete, but your ledger still doesn't tie.
Consumer guidance rarely addresses that operational reality. A single encounter can generate more than one EOB, and reconciling the EOB to the provider bill becomes harder across multiple claims, dates of service, or split facilities, as noted in this discussion of EOB reconciliation complexity.
A workflow that holds up under volume
Use a reconciliation process that forces line-level accountability.
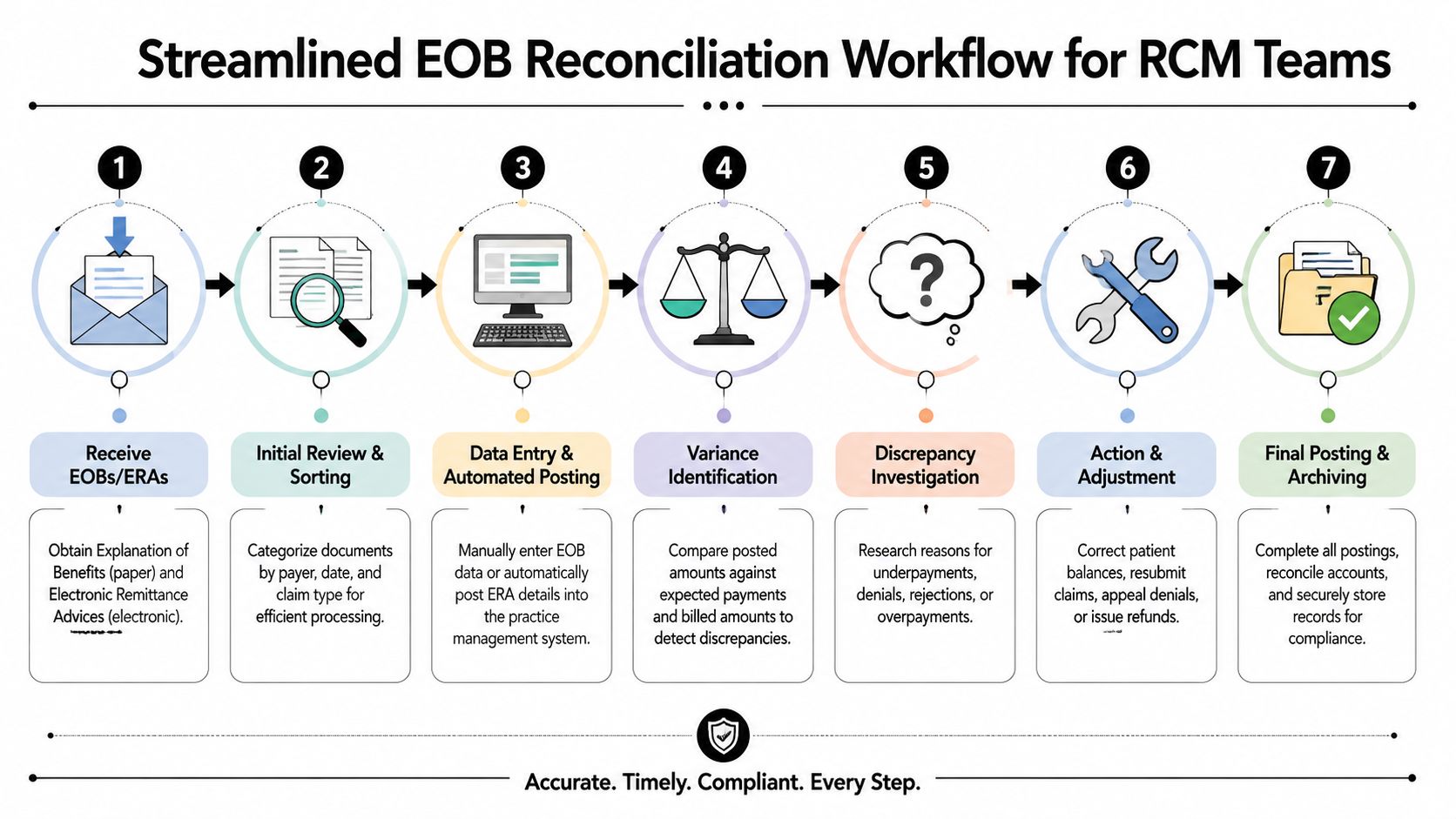
Intake the remit package
Pull the ERA, portal remittance details, payment record, and any available EOB into one work queue. Don't separate them by document type too early.Match at the encounter level first
Confirm patient, payer, date of service, rendering provider, and claim identifiers. If one visit produced multiple claims, group them before posting.Reconcile service lines, not just totals
Each billed line should map to a processed line, even if the payer bundled, split, denied, or repriced it.Validate contractual logic
Review whether the allowed amount and adjustment behavior are consistent with expected pricing logic for that payer and product.Confirm payment movement
Match posted payment to deposit and remittance grouping. A clean adjudication doesn't help if cash application is off.Route exceptions by cause
Authorization, coding, payer pricing, eligibility, coordination of benefits, and missing remit all need different owners.Close only when patient liability is safe to bill
If the adjudication is unresolved, the patient statement should wait.
What works and what doesn't
What works is a queue-based exception model. Posters handle clean claims. A variance team handles mismatches. Contract analysts or senior billers handle true underpayment review.
What doesn't work is asking one payment poster to solve every discrepancy in real time. That slows posting, buries patterns, and turns underpayments into write-offs because the queue gets too old.
Clean posting and strong reconciliation are not the same function. One records the payer's decision. The other tests whether that decision should stand.
Edge cases that need discipline
A few situations cause repeated confusion:
- Bundled services where the payer collapses multiple billed lines into fewer payable lines
- Multiple payers where the primary EOB is present but the secondary balance logic isn't
- Split billing across facility, professional, anesthesia, pathology, imaging, or outsourced specialty components
- Processed but unpaid claims where the payer shows adjudication but the provider's system doesn't show a matching remittance path
When those cases appear, don't force them into a standard posting lane. Build a hold code, require line-item documentation, and assign a named owner. Without that structure, the same unresolved balance gets touched repeatedly and never resolved.
Finding Hidden Underpayments with EOB Analysis
Monday morning, a payment poster clears a stack of claims that look fine on the surface. The payer paid something on each one. No hard denial. No obvious zero-pay line. Thirty days later, cash is short, A/R is aging, and nobody can point to a single catastrophic miss. That pattern is where underpayments live, and the EOB is usually the first document that shows it.
Frontline staff often review EOBs claim by claim. Revenue leaders review them by payer behavior. That shift matters because the EOB ties the payer's adjudication to the financial outcome of the encounter. Blue Shield of California notes that an EOB includes a claim summary and line-level patient responsibility details in its guide to reading an EOB. For providers, those same line items are less about explaining a bill to a patient and more about spotting repeatable reimbursement behavior.
Look for repetition, not isolated variance
One strange adjustment can be noise. The same adjustment logic across one payer, one product, one specialty, one CPT family, or one place of service is a revenue issue that needs ownership.
Organize review around pattern buckets such as:
- Downcoded payment behavior where the payer prices a lower service intensity than the claim supports
- Bundling drift where separately billable services repeatedly collapse into one payable line
- Fee schedule mismatch where allowed amounts do not match expected contract or pricing logic
- Modifier blindness where adjudication ignores the effect of a modifier that should change payment
- Patient responsibility inflation where too much balance shifts to deductible, coinsurance, or non-covered amounts
A good analyst does not stop at “paid” or “denied.” The better question is whether the payer handled similar claims the same way, and whether that logic matches contract terms, policy, and claim construction.
Use codes as clues, not conclusions
CARCs, RARCs, and payer remarks help classify the issue, but they do not settle it. Payers can attach a technically valid reason code to an allowance that still conflicts with your contract, your coding, or the documentation in the record.
When a repeat pattern surfaces, review it through three lenses:
| Question | Why it matters |
|---|---|
| Is the payer's stated reason consistent with the claim details | Stops staff from accepting the code at face value |
| Is the pricing behavior consistent across similar claims | Separates one-off errors from systemic underpayment |
| Does the issue start upstream or at adjudication | Determines whether the fix belongs with registration, coding, billing, or payer follow-up |
That last point saves time. If the same variance appears only on claims with a certain modifier, the problem may sit in coding edits or payer logic. If it appears across cleanly built claims with no upstream defect, the payer becomes the focus.
Where recoverable revenue usually hides
The core issue is not the obvious denial. It is the normal-looking payment that lands below expectation and then gets posted without challenge.
In our experience, the biggest underpayment problems do not announce themselves as denials. They show up as recurring variances that staff can explain away one claim at a time.
Common examples include:
- A payer repeatedly allows less for the same service family even though your contract files show no pricing change
- A reduction appears only when a specific modifier is present
- The facility side and professional side of the same encounter adjudicate under different logic than expected
- A payer pushes more balance to patient responsibility than your team would expect based on prior plan behavior
These issues belong in your healthcare denial management process, even when the claim was not denied outright. If the payer applied the wrong reimbursement logic, the recovery work should follow the same disciplined path as denials and appeals.
Build a payer behavior file
Strong billing departments keep a living record of payer patterns. Not a folder full of PDFs. A structured file that lets the team prove repetition.
Track:
- payer
- plan type
- service category
- place of service
- recurring adjustment logic
- internal owner
- status of dispute or reconsideration
- supporting contract or policy reference
That file changes the quality of your follow-up. A collector arguing one claim often gets a scripted response. A billing manager showing twenty materially similar EOBs, the same reduction pattern, and the contract language behind the expected rate gets a different conversation.
One practical note. If you use an outside revenue partner, ask whether they identify underpayments only at the single-claim level or whether they maintain payer-pattern intelligence tied to appeals and dispute readiness. RevGuard, for example, describes its work as connecting billing operations with underpayment and dispute handling, which fits the operating model this analysis requires.
Turning EOB Insights into Winning IDR Strategies
An EOB by itself doesn't recover revenue. It becomes valuable when your team converts it into evidence.
That evidence starts with adjudication clarity. What did the payer process, what did it allow, what did it deny or reduce, what explanation did it provide, and how does that compare with your internal expectation for the claim? Once you can answer those questions consistently, you're no longer sending generic reconsiderations. You're building claim files that force a specific response.
What a dispute-ready file includes
Strong appeal and dispute files usually have the same backbone:
- The claim record exactly as submitted
- The EOB or equivalent adjudication detail showing the payer's formal position
- The payment record tied to the posting and deposit trail
- Documentation support from the chart, operative report, or service record when relevant
- Contract or pricing support if the issue concerns allowed amount or reimbursement logic
- A variance summary that explains what should have happened and what happened
Notice what's missing. General complaints. Broad statements that the payer underpaid. Those don't move cases.
Turning analysis into argument
A useful underpayment argument is narrow and documented.
Instead of saying the payer paid incorrectly, say that the payer processed a defined service line in a defined way, assigned a specific adjustment or pricing outcome, and created a variance that doesn't align with your claim record, coding, or reimbursement expectation. The EOB gives you the payer's own language to work from.
That precision matters in three settings.
Internal appeal workflows
Your first objective is to make the reviewer's job easy. Show the line, the decision, the variance, and the basis for correction. If your team can't summarize the issue in a few clear sentences with supporting documents attached, the file isn't ready.
Payer negotiations
EOB analysis is useful beyond one-off appeals. When the same issue appears repeatedly, you can aggregate examples and challenge the payer's operational behavior instead of fighting isolated claims forever. That changes the conversation from “please reprocess this claim” to “your adjudication pattern is creating repeat variance in this service category.”
Independent Dispute Resolution
IDR preparation punishes vague documentation. If your upstream billing process is inconsistent, your downstream dispute position weakens.
That's why RCM and dispute strategy should work together from the beginning. A practical example of that operating model appears in how RCM and IDR work together. The core idea is straightforward. Clean, well-documented adjudication analysis creates stronger arbitration files later.
A weak appeal usually starts months earlier, when the team posts the EOB, notes “underpaid,” and saves nothing that proves it.
Trade-offs that matter in the real world
Not every variance deserves the same effort.
Some should be corrected with a simple reconsideration. Some need formal appeal support. Some belong in broader payer escalation because the issue is systemic. And some should be held for dispute pathways where the reimbursement stakes and legal framework justify the work.
The mistake is using one response for every scenario. That burns staff time on low-value disputes and leaves high-value patterns underdeveloped.
A better triage model sorts cases by:
| Case type | Best response |
|---|---|
| Clear posting or mapping error | Correct internally and rebill if needed |
| Isolated payer misread | Reconsideration or focused appeal |
| Repeated pricing or bundling pattern | Escalate with aggregated evidence |
| High-stakes disputed reimbursement | Prepare for formal dispute or IDR pathway |
The operational takeaway
If you want stronger recovery rates, stop treating EOB review as a back-office chore. Treat it as the evidence intake point for enforcement.
The EOB in medical billing gives you the payer's adjudication record. Reconciliation tells you whether the account balances. Pattern analysis tells you whether the payer is behaving consistently. Dispute strategy turns that information into recovered revenue.
RevGuard helps provider organizations connect routine revenue cycle work with dispute-ready reimbursement enforcement. If your team is identifying underpayments but struggling to turn EOB findings into organized appeals, payer challenges, and IDR support, RevGuard is one option to evaluate alongside your existing RCM infrastructure.